
Table of Contents
Introduction: Patient Portals Were Designed for Compliance, Not Care
Patient portals and the patient portal market did not emerge from clinical need. They emerged from regulations.
The modern patient portal is a byproduct of Meaningful Use and, later, the 21st Century Cures Act, policies intended to ensure data access, not care delivery. This origin story matters, because systems tend to remain constrained by the incentives that created them.
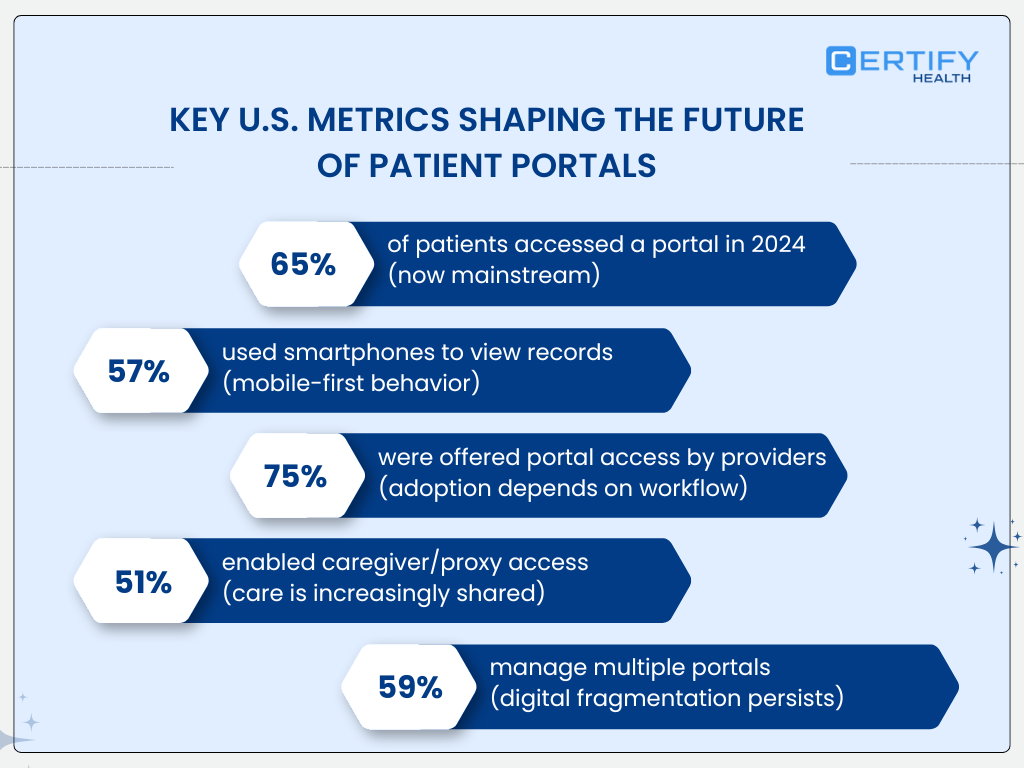
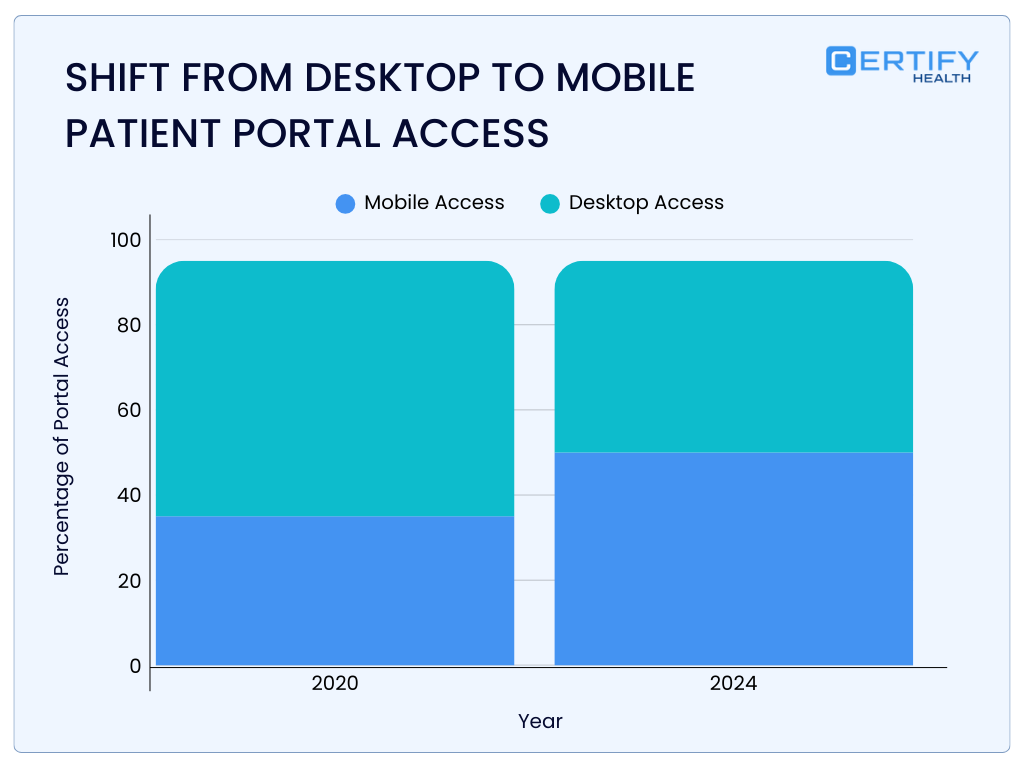
By 2022, over 77% of U.S. patients reported being offered online access to their medical records, yet only about 57% actually accessed them, and far fewer used portals in any sustained or meaningful way.
Government data further shows that only ~30% of patients log into their portal six or more times per year, a threshold that begins to resemble ongoing engagement rather than episodic curiosity.
This gap between access and use is not accidental. It reflects a structural mismatch: portals were built to expose data, not to support decisions, workflows, or financial clarity.
The central claim of this article is deliberately strong:
Medical patient portals, as currently designed, are insufficient for modern healthcare delivery. Until they are reconceived as clinical and financial infrastructure—not compliance artifacts, they will continue to underperform.
What Are Medical Patient Portals?
Traditional Definition (EHR-Centric View)
In federal policy and EHR vendor documentation, a medical patient portal is defined narrowly. It allows patients to:
- View elements of their electronic health record
- Send and receive secure messages
- Schedule or request appointments
- Review laboratory and imaging results
This definition aligns precisely with regulatory language. It does not align with how care actually unfolds.
Peer-reviewed studies repeatedly show that mere access to records does not translate into improved outcomes, nor does it reliably reduce administrative burden.
A large body of U.S. research demonstrates that portal adoption rates plateau quickly, particularly among older adults, patients with lower digital literacy, and those managing complex or behavioral health conditions (PubMed systematic reviews, 2015–2022).
In short: the traditional definition answers what data is visible, not what work is accomplished.
Modern Definition (Care Infrastructure View)
A modern patient portal must be understood not as a viewing layer, but as infrastructure that coordinates clinical, administrative, and financial transactions.
Portals as Transaction Engines (Clinical + Financial)
Healthcare delivery is transactional long before a clinician enters the room. Eligibility checks, intake accuracy, consent capture, and financial responsibility determination all occur upstream, and failures here propagate downstream.
Yet federal data shows that most portals are used primarily for viewing results and messaging, not for completing pre-visit tasks that reduce operational friction. This is a critical missed opportunity.
Research from U.S. health systems demonstrates that incomplete or inaccurate intake data is a major contributor to claim denials, rework, and delayed reimbursement, none of which are meaningfully addressed by read-only portals.
A portal that cannot reliably handle intake, verification, and financial transactions is not infrastructure. It is a dashboard.
Portals as Patient Identity and Data Trust Layers
One of the most under-discussed failures of patient portals is identity fragmentation.
ONC data shows that nearly 60% of U.S. patients maintain more than one patient portal account, often across primary care, specialty care, and hospital systems. This multiplicity creates inconsistent demographic data, duplicated histories, and fractured trust.
From a systems perspective, this is indefensible. Identity should be persistent across the patient journey. Instead, portals replicate silos.
The consequence is not merely inconvenience. Identity fragmentation directly undermines data integrity, consent management, and patient confidence, especially when clinical, billing, and messaging systems are misaligned.
Portals as Workflow Extensions, Not Standalone Tools
A portal that exists outside operational workflows increases workload rather than reducing it.
Multiple U.S. studies show that secure messaging volume increases clinician and staff burden when messages are not triaged or contextualized, leading to burnout rather than efficiency gains. When portals are not embedded into scheduling, intake, billing, and follow-up workflows, they become parallel systems that require reconciliation.
In its modern form, it should be a workflow extension that collapses handoffs.
The Hidden Problem with Most Medical Patient Portals
1. Built for Systems, Not Humans
Patient portals overwhelmingly reflect how EHRs store data, not how patients process information.
Peer-reviewed U.S. research shows that patients with limited health literacy struggle significantly with portal navigation and comprehension, even when access is technically available. Interfaces expose raw lab values, ICD-coded problem lists, and clinician-centric terminology with minimal interpretation.
This design choice has measurable consequences:
- Increased anxiety after result release
- Higher message volume seeking clarification
- Increased call center utilization
These are not usability quirks. They are systemic design failures rooted in EHR-first thinking.
2. Adoption Metrics Are Misleading
Healthcare organizations frequently report portal “success” using activation and login metrics. This is a category error.
Meta-analyses of U.S. studies show that average real-world portal adoption hovers around 20–30%, despite higher rates reported in controlled pilots. Even among adopters, usage is episodic, often clustered around acute events rather than longitudinal care.
Critically, login frequency correlates poorly with clinical outcomes. A patient logging in to view a lab result once a year is counted the same as one managing a chronic condition weekly.
Until organizations measure task completion, error reduction, and workflow impact, adoption metrics will remain misleading.
3. Fragmentation Across the Patient Journey
In most U.S. health systems:
- Intake lives in one system
- The portal lives in another
- Billing lives somewhere else entirely
Federal interoperability efforts have improved data exchange, but they have not unified experiences. Patients routinely re-enter demographic data, repeat insurance information, and navigate multiple payment pathways.
From a systems engineering perspective, this fragmentation guarantees inefficiency. From a patient perspective, it signals disorganization.
A portal that does not unify the patient journey is not a front door. It is a corridor.
What Patients Actually Expect from Medical Patient Portals (But Rarely Get)
1. One Identity, One Experience
Patients do not think in terms of modules. They expect continuity.
U.S. survey data consistently shows that patients abandon digital tools when they are forced to manage multiple identities, credentials, and interfaces. The fact that a majority of portal users maintain more than one account is evidence of structural failure.
A modern portal must act as a persistent identity layer that spans clinical, administrative, and financial interactions.
2. Clarity Over Access
Access without interpretation shifts cognitive labor to patients.
Research shows that patients value explanations and next steps more than raw data, particularly after abnormal test results. When portals fail to provide context, they increase anxiety and downstream utilization, ironically negating efficiency gains.
Clarity is not a “nice to have.” It is a safety issue.
3. Real-Time Financial Transparency
Financial uncertainty remains one of the strongest deterrents to care.
Despite federal price transparency rules, most patient portals still do not provide actionable cost information prior to services. This disconnect contributes to delayed care, surprise billing disputes, and unpaid balances.
A portal that ignores the financial dimension of care is incomplete by design.
Clinical Impact of Medical Patient Portals
Where Portals Improve Outcomes
U.S. studies show that portal use is associated with:
- Improved medication adherence
- Increased preventive screening completion
- Higher patient-reported satisfaction and self-efficacy
However, these benefits are context-dependent. They appear most consistently in chronic disease management where portals are integrated into longitudinal workflows.
Where Portals Fall Short
Evidence linking portals to hard clinical outcomes like hospitalizations, disease control metrics, mortality, is inconsistent.
Systematic reviews show that less than half of studies demonstrate measurable clinical improvement, and many show no effect at all. This does not indict portals as a concept; it indicts their design.
Tools that expose data without shaping behavior should not be expected to change outcomes.
Why Context Matters More Than Features
Secure messaging without triage increases workload. Results without interpretation increase anxiety. Scheduling without eligibility confirmation increases denials.
Context is the missing layer. Features alone do not produce value.
Financial and Operational Impact: The Overlooked Role of Patient Portals
Intake Errors Start Before the Visit
Revenue cycle failures frequently originate upstream.
Demographic inaccuracies, eligibility mismatches, and authorization gaps are well-documented drivers of claim denials in U.S. healthcare. Yet most portals do little to validate or reconcile this data in real time.
This is a design failure with direct financial consequences.
Portals as Revenue Leakage Controls
When portals are integrated into intake, eligibility verification, and payment workflows, they can reduce leakage by:
- Improving data accuracy
- Capturing patient responsibility earlier
- Reducing downstream rework
This requires treating the portal as financial infrastructure, not a messaging tool.
Why Most Portals Don’t Reduce AR Days
The answer is simple: they are not connected to billing systems in a meaningful way.
Disconnected payment flows, delayed statements, and manual reconciliation persist because portals were never designed to close the revenue loop.
Medical Patient Portals vs the Digital Front Door
Portal = Access Layer
Digital Front Door = Orchestration Layer
A digital front door coordinates identity, intake, eligibility, clinical communication, and payment into a single experience.
Most portals do none of this well.
Security, Privacy, and Trust
HIPAA |
Authentication Fatigue |
Trust as a Design Outcome |
How to Evaluate Medical Patient Portal Software
Questions That Matter
- Does this reduce total system work?
- How are errors surfaced and corrected?
- Can it handle real-world payer complexity?
2026 Baseline Capabilities
- Embedded intake and verification
- Real-time benefits clarity
- Integrated payments
- Bi-directional EHR synchronization
Red Flags
- Feature density without workflow impact
- Engagement metrics without outcome linkage
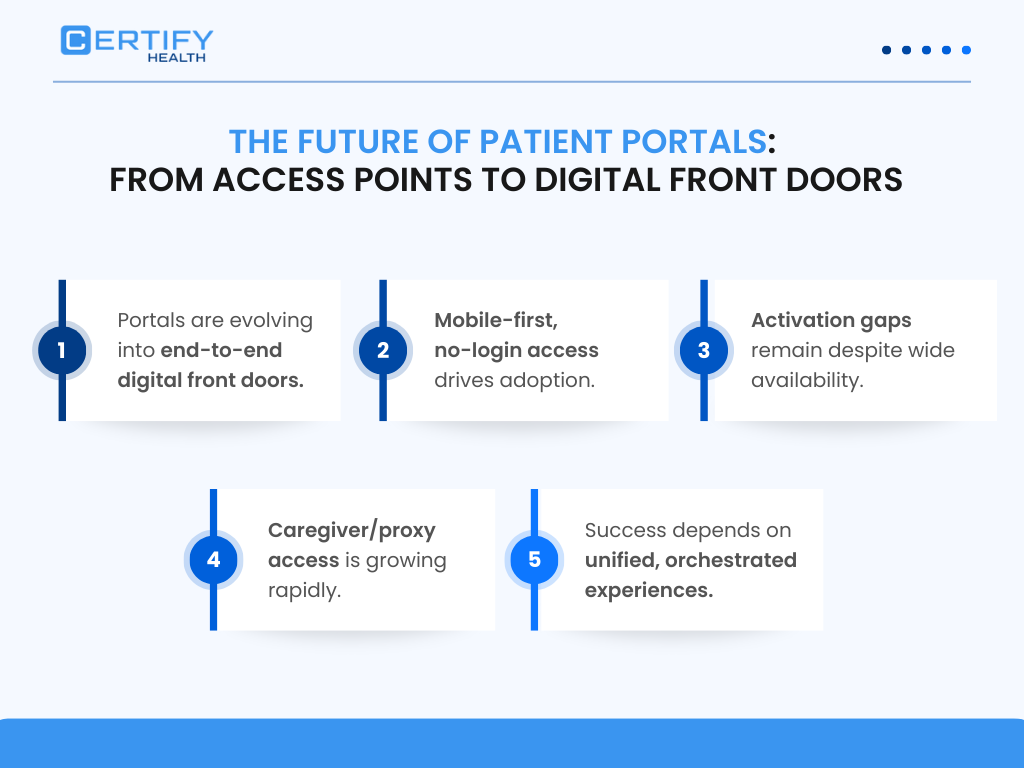
The Future of Medical Patient Portals
Portals will disappear as standalone products.
They will be absorbed into patient operating systems…event-driven, AI-mediated, and embedded across care delivery.
AI’s role will be interpretation, not automation. Care will become continuous, not visit-bound. There will also be enough emphasis on trust portals real-time access compliance artifacts.
Final Take
The patient portal, as originally conceived, has reached its limits.
Healthcare does not need better dashboards. It needs infrastructure that unifies care delivery, reduces friction, and aligns clinical and financial realities.
That is the future of the digital front door.
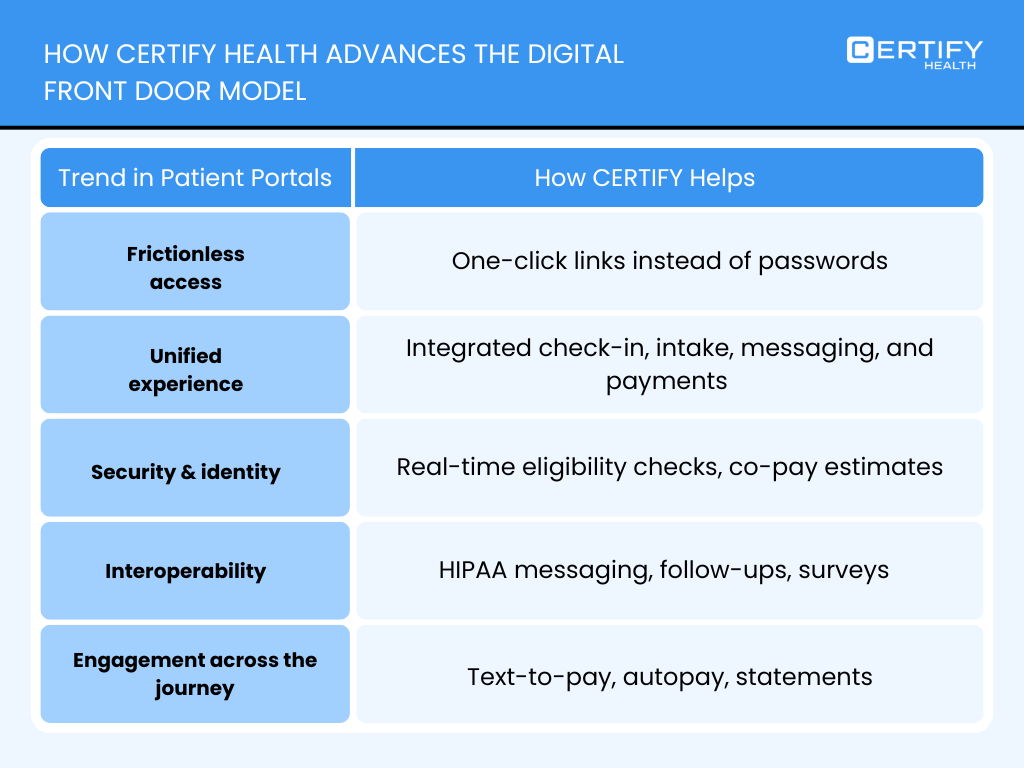
Where CERTIFY Health Fits
Platforms like www.certifyhealth.com represent this infrastructure-first approach, treating the patient front door not as a portal, but as a coordinated system for intake, eligibility, payments, and workflow unification.
CERTIFY Health has been highlighted as one of the most secure healthcare patient portals 2025 2026, and has appeared in the top results for patient portal usability rankings 2025 and 2026.
The next era of patient engagement will not be defined by logins. It will be defined by measurable outcomes, operational clarity, and trust at scale.




















