
Table of Contents
- The CMS Prior Authorization rule from the Centers for Medicare & Medicaid Services will change how prior authorizations are handled across the entire revenue cycle, not just IT systems.
- The January 1, 2027 deadline for the Prior Authorization API means organizations need to prepare now to avoid workflow disruption and compliance risk.
- Automating prior authorization can reduce denials, save staff time, and improve cash flow, making it both an operational and financial priority.
43. That’s how manyprior authorization requests the average physician completed every single week in 2024.
That’s roughly 12 hours of staff time, gone. Not on patient care. On paperwork.
(Source: AMA Survey, via Becker’s Payer Issues)
For revenue cycle teams, those hours add up fast.
Faxes, insurance portals, and endless phone tags that remain unattended.
The prior authorization process has been broken for years. And the cost, to your staff, your budget, and your patients, keeps growing.
Now, that’s changing.
January 2024 marked a major policy update.
The Centers for Medicare & Medicaid Services rolled out the Interoperability and Prior Authorization Final Rule (CMS-0057-F).
This rule was mandated to modernize how prior authorizations are handled.
It requires certain payers to build a CMS Prior Authorization API. This means prior authorization requests and decisions move digitally, in real time.
No more faxes. No more waiting on hold.
This isn’t just a tech update for your IT team. It will change how your entire revenue cycle runs. It will affect your staff, your denial rates, and your bottom line.
Why Prior Authorization Is Broken (By the Numbers)
Prior authorization challenges are not small problems. They cost time, money, and staff morale. Here’s what the data shows.
The American Medical Association ran a survey in 2024. Here’s what they found:
- Doctors handle 39 prior authorization requests per week on average
- That takes about 13 hours of their time each week
- 93% of doctors say prior auth delays care for their patients
- 89% say it leads to burnout
- 1 in 3 doctors say their requests are often denied
The money side is just as bad. The 2024 CAQH Index Report found that prior auth costs the healthcare system $1.3 billion a year.
These numbers aren’t just stats. They’re your team’s daily reality.
What Is the CMS Prior Authorization API?
The CMS Prior Authorization API is a digital tool. It lets payers and providers share prior authorization data in real time.
No faxes. No phone calls. No payer portals.
It’s built on a FHIR-based API standard.
FHIR stands for Fast Healthcare Interoperability Resources. It’s the same standard used across the CMS interoperability ecosystem. It helps data move in a clean, digital format.
This is a big step forward for healthcare interoperability in the U.S.
Under CMS-0057-F, payers must build a Prior Authorization API that does four things:
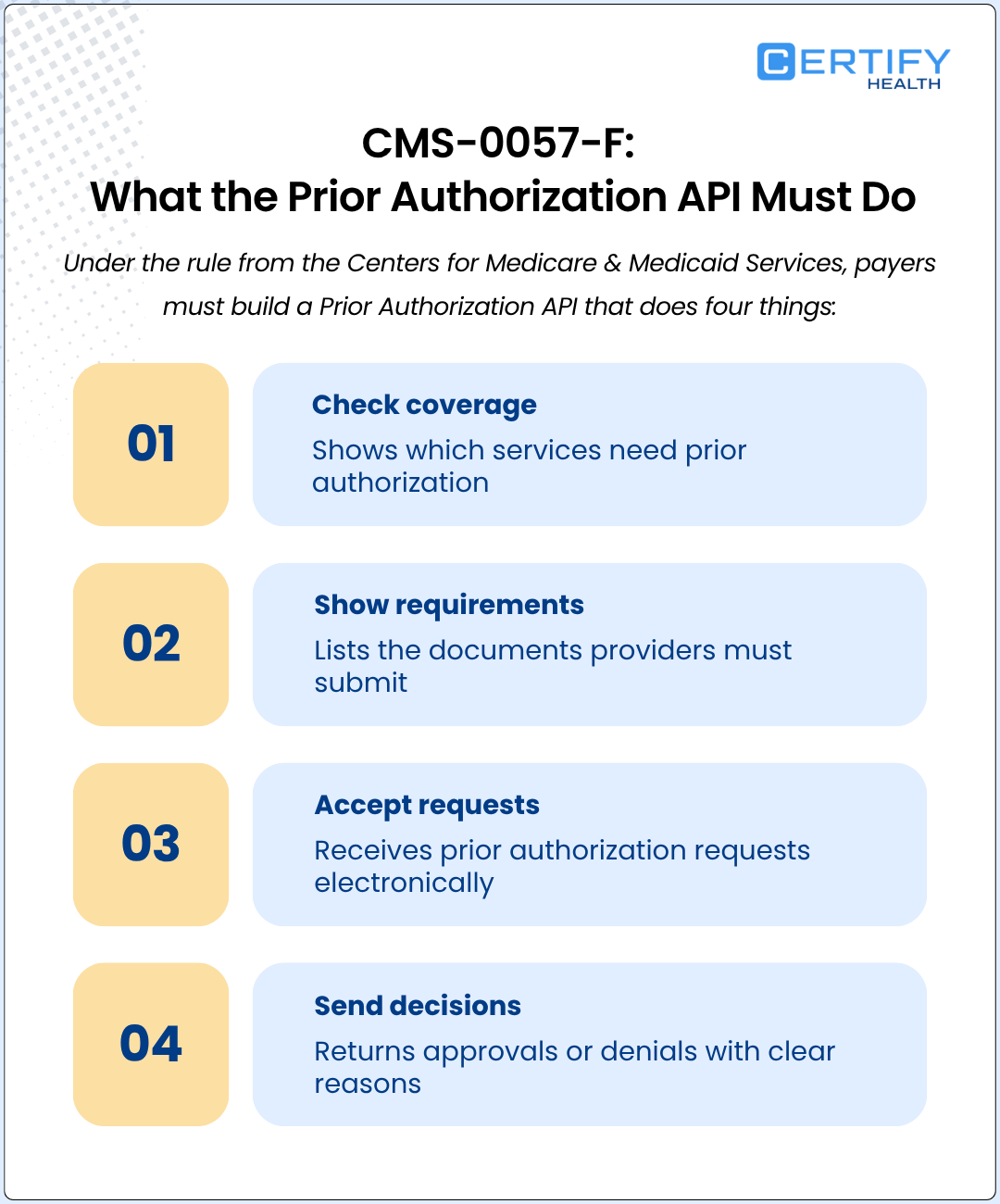
- Lists covered services: Tells providers which services need prior authorization
- Shows required documents: Tells providers what clinical records to submit
- Accepts digital requests: Receives prior authorization requests through a standard healthcare API integration
- Sends digital decisions: Returns approvals or denials with clear reasons
The technical standard is HL7® FHIR® Release 4.0.1. This is the backbone of the whole CMS interoperability system.
Who Has to Comply, and By When?
The Prior Authorization Final Rule does not apply to every payer. It targets a defined group of health plans.
Does your organization partner with any of them? Then you’re in scope.
- Medicare Advantage plans and Medicare Advantage organizations
- State Medicaid and CHIP fee-for-service programs
- Medicaid managed care plans
- CHIP managed care entities
- Qualified Health Plans (QHPs) on Federal Exchanges
Medicare Advantage plans are growing fast. Over 33 million people are enrolled today. If your org handles a lot of Medicare prior authorization, this rule hits close to home.
Here are the key deadlines:
| Date | What Must Happen |
|---|---|
| January 1, 2026 | Payers must make decisions faster. 72 hours for urgent requests. 7 days for standard ones. Payers must also start reporting prior authorization data publicly. |
| March 31, 2026 | Payers must post their first public report on prior auth metrics for 2025. |
| January 1, 2027 | Full API deadline. The Prior Authorization API, Patient Access API, Provider Access API, and Payer-to-Payer API must all be live. |
| Hygienists / Assistants | Protect screens, document carefully, access only the charts they need. |
| Billing / Insurance | Use HIPAA compliant hosting and portals, avoid fax‑to‑email shortcuts, follow data breach response steps. |
January 2027 is not as far off as it sounds.
If your team hasn’t begun preparing yet, this is the moment to get started.
How the Prior Authorization API Actually Works
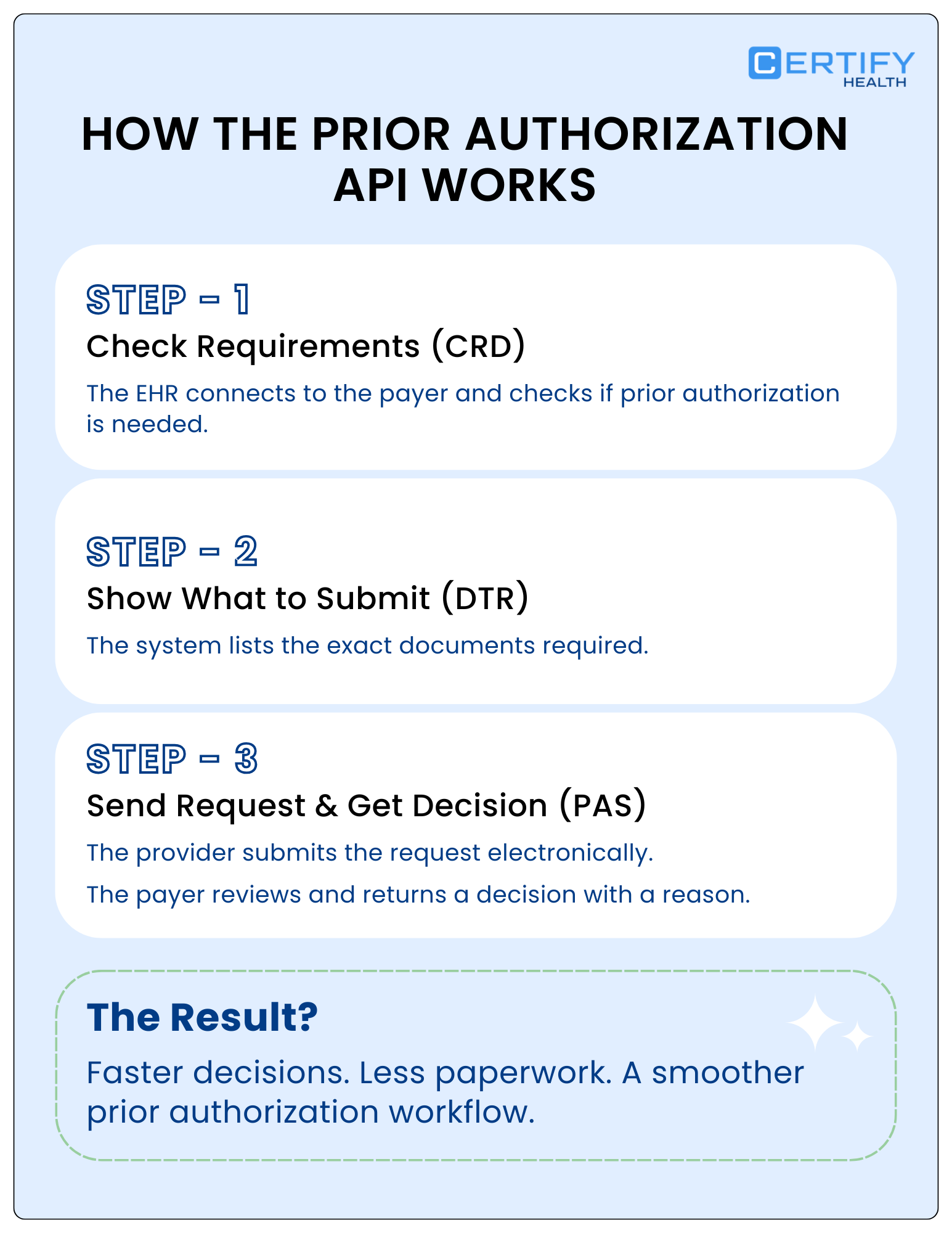
The CMS Prior Authorization API works in three steps. Your revenue cycle and IT teams need to know each one. The prior authorization workflow looks like this:
Step 1 — Coverage Requirement Discovery (CRD)
A clinician orders a service. The EHR instantly connects to the payer using a FHIR-enabled API and checks requirements.
It confirms, right then, whether prior authorization is needed.
No manual lookup. No phone call. No fax.
Step 2 — Documentation Templates and Rules (DTR)
Auth is needed? The Prior Authorization API tells the provider exactly what to submit. Staff can pull the right forms before they send the request.
This cuts down on missing documents. It also reduces denials.
Step 3 — Prior Authorization Support (PAS) via the PARDD API
The provider sends the request through their EHR. The PARDD API handles the exchange. PARDD stands for Prior Authorization Requirements, Documentation, and Decision.
The payer reviews the request and sends back a decision. It may be an approval, a denial with a reason, or a request for more info. It all happens within the federal time limits.
The PARDD framework ties CRD and DTR together into one smooth prior authorization workflow.
The Result?
A prior authorization process that used to take days can now be done in hours. The decision goes straight into the patient’s record.
Why Revenue Cycle Leaders Should Care
The CMS Prior Authorization rule isn’t just an IT project. Prior authorization challenges hurt your bottom line. They slow down care. They drain your staff. The API is built to fix that.
What it means for your team is right here:
Fewer Denials From The Start
The API shows your team what the payer needs before you submit. That means fewer missing documents. Fewer denials. This is the biggest financial win of prior authorization automation.
Less Manual Work Through Clinical Workflow Automation
Many practices have staff who do nothing but chase prior auths. AMA data says 40% of practices hire full-time staff just for this. Prior authorization automation and clinical workflow automation can free up those people. They can move to higher-value work.
Clearer Reasons for Denials
Starting in 2026, payers must give a clear reason for every prior authorization denial. Right now, denial codes are often vague. This change will help your team write better appeals. It will also help you spot patterns and fix root causes.
Better Data on Payer Performance
Payers must report prior authorization data each year. That means approval rates, denial rates, and decision times, all public. You can use this data to benchmark payers. It’s especially useful for Medicare Advantage plans, where auth volume is high.
What This Means for Healthcare Providers Today
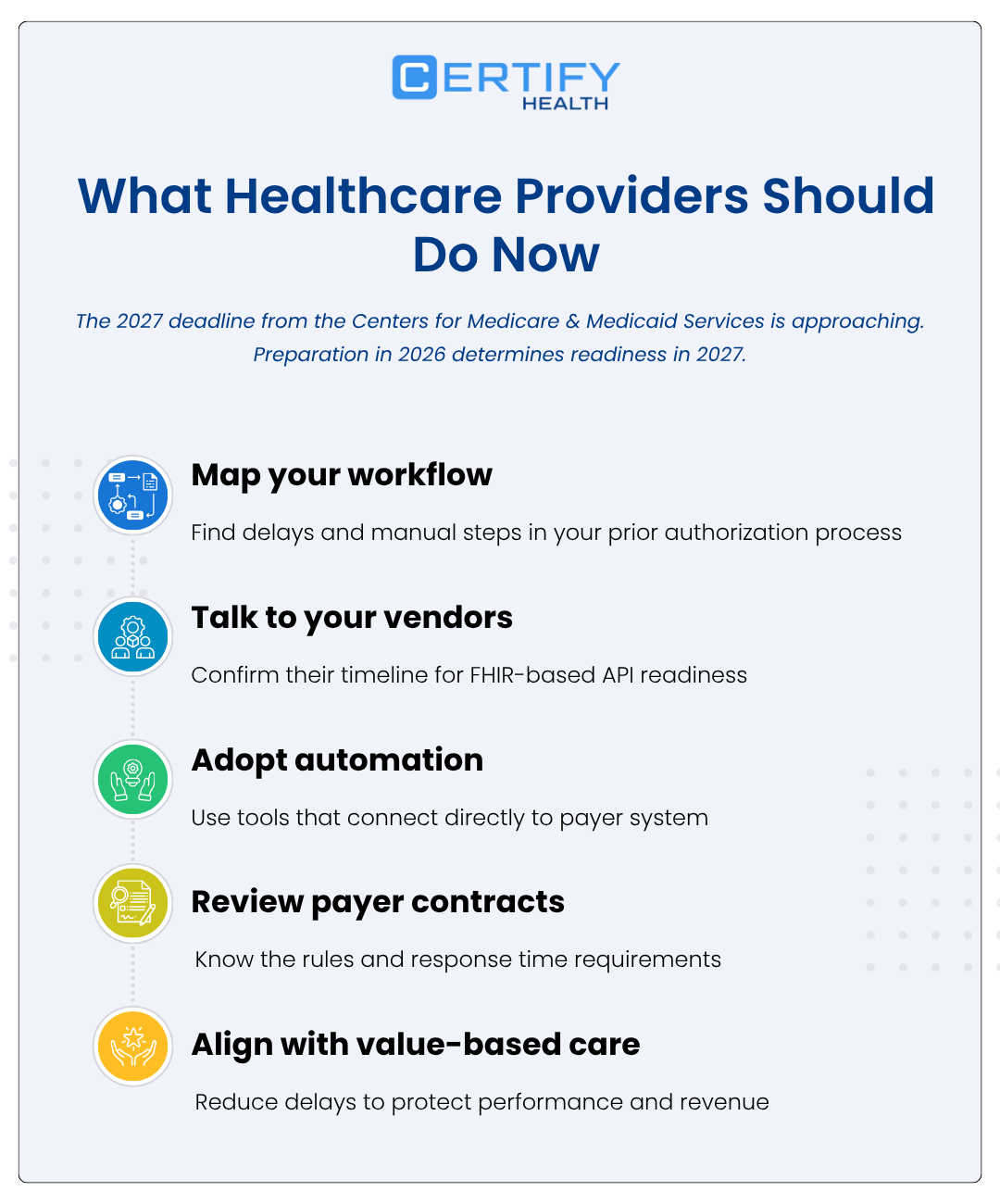
The 2027 deadline is coming. The groundwork needs to start now. Here’s what revenue cycle leaders should do in 2026:
1. Map Your Prior Authorization Process
Look at your current prior authorization workflow step by step.
- Where does it slow down?
- Where are people doing things by hand?
This map will show you where to focus. It also helps you build the case for automated prior authorization software.
2. Talk To Your EHR And Tech Vendors
A healthcare interoperability platform built for CMS-0057-F needs strong EHR support.
- Talk to your technology partners and find out how they plan to meet these new requirements.
- Find out where you are in their timeline.
If a vendor has no clear path to FHIR-based API support by 2027, that’s a risk.
3. Look At Automated Prior Authorization Software
The new Prior Authorization API model works best with automated prior authorization software.
Tools with built-in healthcare API integration will connect to payer systems much faster. Manual workflows will fall behind.
4. Check Your Payer Contracts
Payers now have to meet federal time limits for prior authorization decisions.
- Review your contracts.
This is key for Medicare prior authorization and Medicare Advantage plans.
- Know what you can do if a payer doesn’t meet the rules.
5. Connect prior Auth to Value-based Care
The Prior Authorization API fits into the bigger shift toward value-based care.
In a value-based care model, delays and denials hurt your performance scores. They also affect shared savings.
Less prior auth friction means better outcomes on both fronts.
6. Start Your Digital Health Transformation Now
Digital health transformation can’t wait if you’re subject to CMS-0057-F.
It’s not a future project. It’s a current need.
Health systems that invest in healthcare interoperability today will be ready in 2027. Those that wait will be racing the clock.
How CERTIFY Health Supports Prior Authorization Readiness
CERTIFY Health is built for the modern revenue cycle. Our platform meets CMS interoperability rules, including the CMS Prior Authorization mandate under CMS-0057-F.
As a healthcare interoperability platform, CERTIFY Health helps your team:
1. Automate front-end prior authorization workflows
So, staff spend less time on paperwork.
Cut manual steps through prior authorization automation at patient access and move patients through registration faster.
2. Connect through FHIR-based APIs
So, your systems talk to payers automatically.
Our healthcare API integration supports the PARDD API and all interoperability capabilities required by the final rule, reducing portal logins and data re-entry.
3. Stop denials before they happen
So, you get paid faster.
We check eligibility and documentation completeness upfront. This works like built-in automated prior authorization software inside your intake process.
4. Enable clinical workflow automation
So, teams always know the status.
Your clinical and revenue cycle staff receive real-time prior authorization updates inside the tools they already use.
5. Support value-based care goals
So, you improve outcomes while controlling costs.
Less administrative friction means smoother operations, better patient flow, and stronger shared savings results.
The prior authorization landscape is evolving quickly. Moving to digital health is no longer a choice, it’s a necessity. Health systems that act now will be in a much stronger place.
The Bottom Line
The CMS Prior Authorization API is not a background IT task. It’s a federal rule. It’s rooted in CMS-0057-F and the Prior Authorization Final Rule. It will change how every prior authorization is sent, tracked, and resolved, across Medicaid, and across all Medicare Advantage plans.
Think of this blog as your prior authorization guide to what’s coming. Learn the rule. Check your readiness. Take action now. The teams that invest in healthcare interoperability, prior authorization automation, and FHIR-based API tools today will be ahead of the curve in 2027.
The CMS Prior Authorization mandate is coming for every health system. And the question is – Are you ready for it?
Want to see how CERTIFY Health’s healthcare interoperability platform helps you prepare for CMS-0057-F?




















