
Table of Contents
Why the FY 2027 SNF Proposed Rule Matters
CMS released the FY 2027 SNF PPS proposed rule on April 2, 2026. It went into the Federal Register on April 7, 2026.
This rule comes out every year. It updates Medicare payment policies for skilled nursing facilities. It also sets new quality rules and scoring goals. In short, it affects your Medicare reimbursement, your staff, and your compliance duties all at once.
You can read every provision in the official CMS fact sheet for CMS-1843-P, published April 2, 2026.
Many SNF operators wait for the final rule before they act. That can be a costly mistake. CMS is accepting comments at this time. This is your chance to push back on changes that could hurt your facility.
CMS set the public comment deadline at June 1, 2026. You can file comments directly at regulations.gov or work through your state or national group. Don’t miss this window.
The final rule is due in late July or early August 2026. It kicks in on October 1, 2026 — the start of federal fiscal year 2027.
The preparation period is limited, so now is the time to act.
Notable Changes in the FY 2027 SNF Payment Proposal
Payment Rate Changes
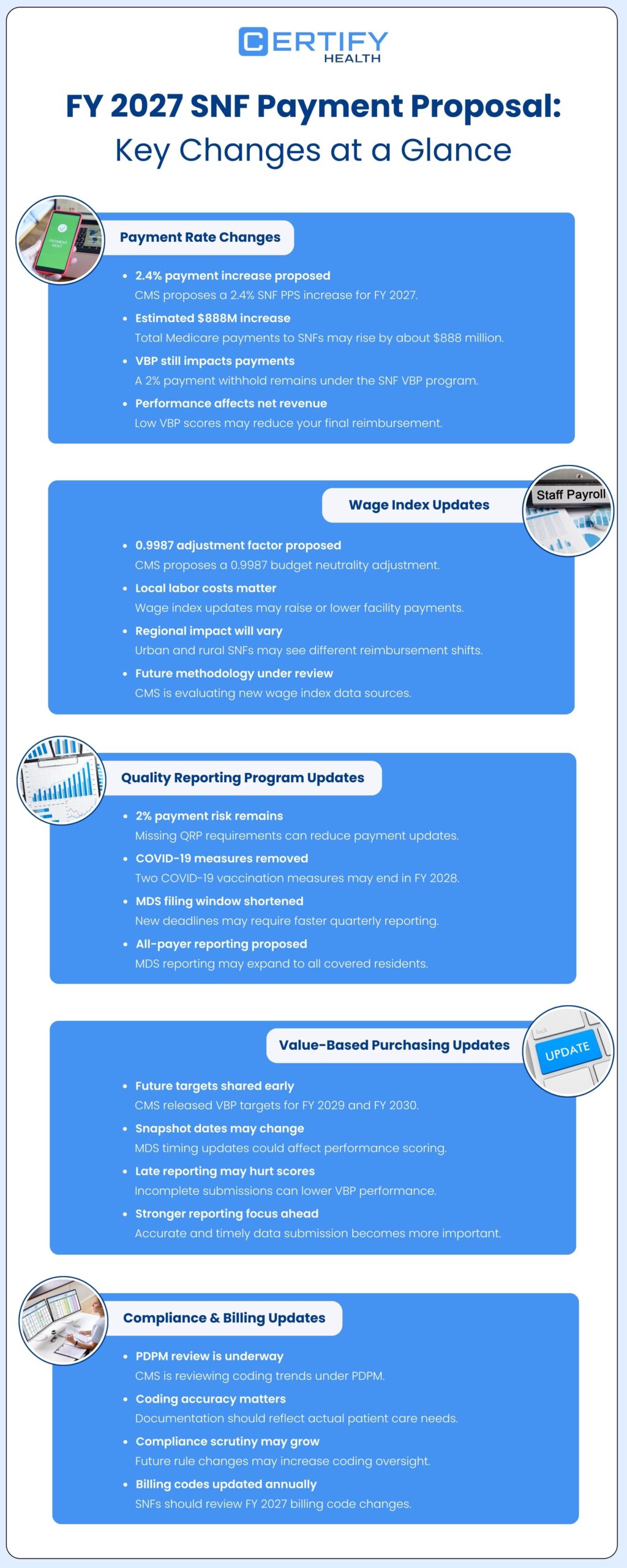
CMS is proposing a 2.4% increase in FY 2027 SNF PPS reimbursement rates. That figure comes from a 3.2% market basket increase, minus a 0.8% productivity adjustment. The CMS SNF PPS, formally called the prospective payment system, is the model CMS uses to set daily Medicare rates for skilled nursing care.
Across all SNFs, CMS estimates this adds up to roughly $888 million in additional Medicare payments for FY 2027. That sounds like good news. But the headline rate is not your net rate.
The SNF Value-Based Purchasing (SNF VBP) program withholds 2% of each SNF’s Medicare Part A fee-for-service payments. CMS then pays back 50% to 70% of that pool as bonus payments, based on how well each facility scores. The SNF VBP reduction is estimated at $203.41 million for FY 2027. That money does not go back to every facility equally.
If your SNF VBP scores are low, your net payment could fall, even with a rate increase on paper.
Wage Index Updates
CMS also proposes wage index changes as part of the SNF PPS refresh. For FY 2027, the proposed budget neutrality adjustment factor is 0.9987. This small adjustment keeps the total payment pool neutral across all SNFs while local rates shift up or down.
These changes reflect what workers earn in your area. They affect the labor portion of your daily Medicare rate. Urban and rural facilities may see very different results. Don’t assume the national 2.4% figure applies to your facility.
CMS is also seeking input on alternative data sources for a future SNF-specific wage index. Options include BLS labor data and cost reports from other care settings. If this moves forward, it could change how your local rate is set. Watch for it in future rule cycles.
Quality Reporting Program Updates
The SNF Quality Reporting Program (SNF QRP) is a pay-for-reporting program. Miss its rules, and CMS cuts your Annual Payment Update by two full percentage points. A paperwork gap can turn into an expensive mistake fast.
Here is what CMS proposes for the SNF QRP:
Two COVID-19 measures will be removed, starting with the FY 2028 SNF QRP:
- COVID-19 Vaccination Coverage among healthcare personnel
- COVID-19 Vaccine: Percent of patients/residents who are up to date
The filing window will get shorter. SNFs currently have 4.5 months to send in Minimum Data Set (MDS) data after a quarter ends. Starting with the FY 2029 SNF QRP, that window shrinks. Data must be in by the 15th day of the second month after each quarter ends. This means less time for your MDS team to complete and check records before the deadline.
MDS filing will expand to all payers, but not right away. CMS proposes requiring MDS data on every SNF resident receiving covered skilled care, regardless of who pays, beginning with the FY 2031 SNF QRP. Right now, MDS data is tied to Medicare and Medicaid claims only. This change will add volume to your MDS process. Plan for it now, even though the start date is a few years out.
CMS also issued a Request for Information (RFI) on advance care planning (ACP). ACP is the ongoing process of writing down a patient’s care wishes before they can no longer speak for themselves. CMS is thinking about adding it as a future SNF QRP measure. This signals a bigger push toward post-acute care coordination and patient-centered records. It is worth tracking closely.
Value-Based Purchasing Updates
For the SNF VBP program, CMS is sharing target performance levels for FY 2029 and FY 2030. This gives your facility more lead time to plan ahead.
CMS also proposes to update the “snapshot date” for two specific MDS-based measures: Discharge (DC) Function and Major Injury (Long-Stay). A “snapshot date” is the point in time CMS pulls MDS data to calculate your performance score. Moving it keeps these two measures in sync with the new, shorter QRP filing deadlines. If your MDS data is late or incomplete on the snapshot date, your score will reflect that. On-time filing matters more than ever.
New Reporting and Compliance Expectations
CMS issued an RFI on updating the Patient-Driven Payment Model (PDPM). The Patient-Driven Payment Model sets how Medicare pays SNFs based on each patient’s clinical needs, not just therapy minutes. The concern CMS raises is called case-mix creep. This is when patient coding drifts toward higher-paying groups over time, without a real rise in care needs. It can happen by accident or by intent.
On October 1, 2019, PDPM officially replaced the previous RUG-IV payment model. CMS has tracked coding trends since then. This RFI signals that PDPM changes may come in future rule years. Review your coding now. Make sure it reflects actual patient need, not just maximum payment. Strong compliance requirements around coding accuracy will matter more if CMS acts on this RFI.
CMS also makes its annual update to consolidated billing for SNFs, refreshing the list of excluded procedure codes for FY 2027. While this is a routine update, your billing team should review the revised code list before October 1.
How These Proposed Updates May Impact Your Facility

Revenue Impact
A 2.4% rate increase is welcome. But your real result rests on three factors: your wage index, your SNF VBP bonus payment, and whether you meet all SNF QRP filing rules. If any one of those goes the wrong way, your Medicare reimbursement could stay flat — or fall. Your revenue cycle team needs to look at all three together, not just the headline rate.
Staffing Pressure
More MDS records. Shorter filing windows. Possible PDPM changes. All of that adds up to more work for your MDS staff, clinical team, and compliance leads. Many facilities are already running lean. More volume without more support creates real risk. Start planning now, whether that means hiring, training, or using better tools.
Documentation Burden
The minimum data set has always been important. It’s becoming more so. CMS is expanding who it covers. It’s cutting the time you have to file it. And it’s watching the PDPM coding that drives your payment rates.
One wrong entry in an MDS record can hurt your payment, your quality scores, and your Care Compare rating — all at once.
This is where hospital-to-SNF handoffs matter most. When a patient moves from a hospital to your SNF, the data you collect at intake shapes the MDS record directly. Gaps in patient intake and eligibility routing, a wrong payer, a missed diagnosis, a skipped prior auth — ripple through the whole care record. Clean intake means accurate MDS records. Accurate MDS records protect both your PDPM coding and your revenue.
Quality Reporting Workflows
The shorter QRP filing window will pressure every SNF. Facilities with paper-based or split workflows will feel it most. Strong scheduling and visit management, where clinical visits link directly to MDS completion, cuts the risk of missed filings. Real-time monitoring and engagement tools that flag open MDS records before the snapshot date will shift from nice-to-have to need-to-have.
4 Actions SNFs Should Take Before the Rule Is Finalized
The rule is not final yet. But October 1 arrives fast. Here is where to focus now.
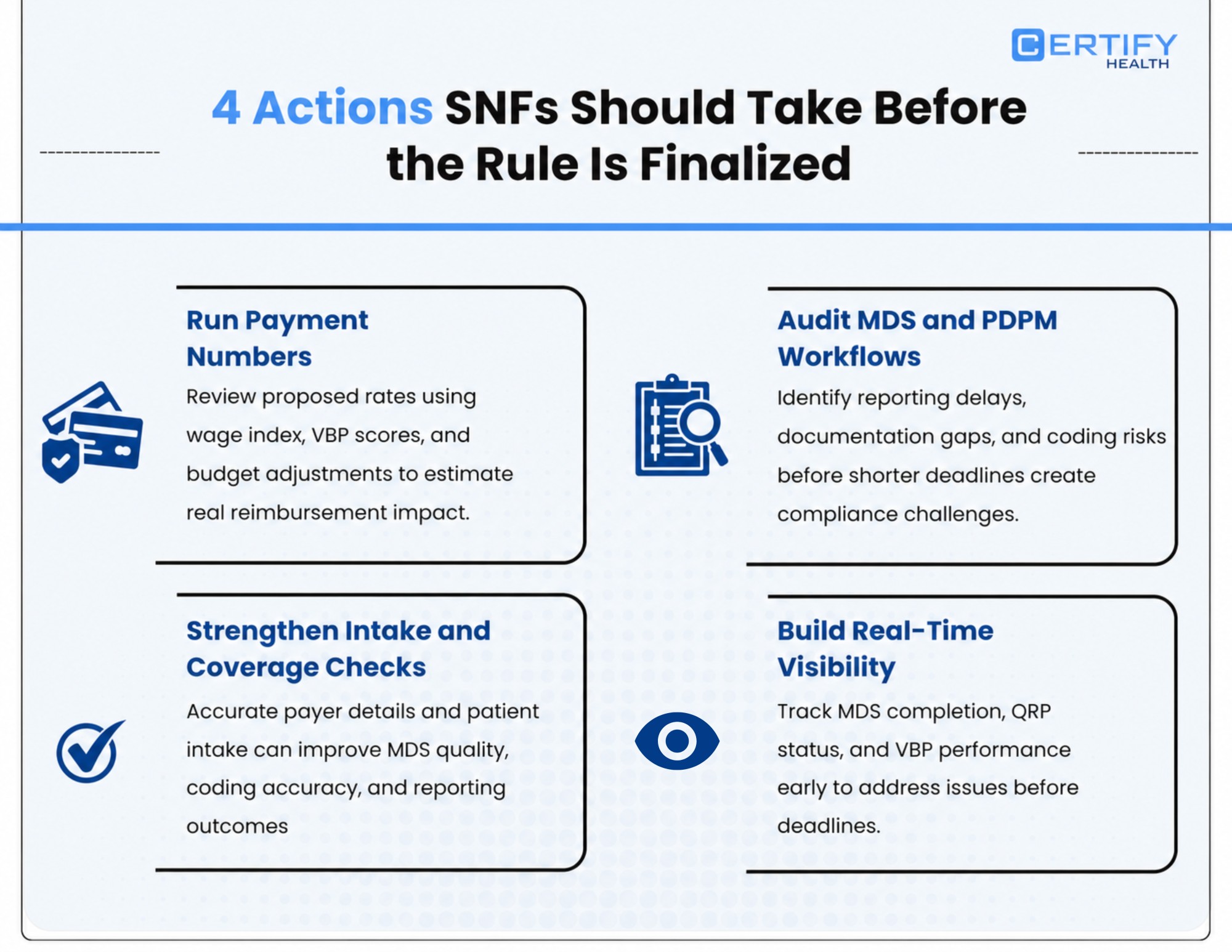
1. Run Your Payment Numbers
Don’t wait for the final rule. Use the proposed 2.4% rate as your base. Then apply your current SNF VBP scores, your local wage index, and the 0.9987 budget neutrality factor. The combined result may differ a lot from the national average. Your revenue cycle team should lead this analysis — and start soon.
2. Audit Your MDS Workflows and PDPM Coding
Walk your current MDS process from start to finish. Where do delays happen? Where do errors show up? Can your team hit the shorter filing deadline? Can it absorb the coming all-payer volume by FY 2031? Find the gaps now, while you still have time to close them. Also review your PDPM coding for signs of case-mix creep, even if it’s unintentional. If CMS sees a pattern in your classification data, you want to catch it first.
3. Tighten Your Intake and Coverage Checks
Strong records start at the front door. When patient intake and eligibility routing is accurate — right payer, right coverage, right clinical baseline — every step after gets easier. Your MDS is cleaner. Your PDPM coding holds up. Your QRP data is more reliable. Better care coordination between hospital discharge teams and your admissions staff reduces hand-off errors and closes gaps that show up later in audits.
4. Build Real-Time Visibility Before October
You cannot fix what you cannot see. Facilities that track MDS completion, QRP filing status, and VBP scores in real time catch problems while there is still time to act. Build that view now, not in late September. Test it. Train your team. Make sure it covers the MDS snapshot dates for DC Function and Major Injury (Long-Stay).
How CERTIFY Health Fits Into This
When compliance requirements tighten — shorter MDS windows, wider filing scope, tighter VBP benchmarks — the gap between well-run and struggling SNFs grows fast.
CERTIFY Health is built for exactly this. The platform links patient intake and eligibility routing, care coordination, scheduling and visit management, transition workflows, and real-time monitoring and engagement into one connected workflow. Your clinical and admin teams always work from the same data.
Nothing falls through the cracks between admission and MDS filing. For SNFs managing the FY 2027 SNF PPS changes, that kind of view across the whole care journey, from intake to post-acute care coordination to quality reporting, is what turns a compliance deadline into a routine task, not a fire drill.
What Happens Next?
Public comment deadline: June 1, 2026. Submit at regulations.gov (Docket ID: CMS-1843-P).
Final rule expected: Late July or early August 2026.
Effective date: October 1, 2026.
Your Pre-October Checklist
- Model net payment impact: 2.4% rate + VBP adjustment + wage index + 0.9987 neutrality factor
- Check wage index changes for your market
- Map your MDS filing workflow and find capacity gaps
- Review PDPM coding for case-mix creep patterns
- File public comments by June 1, 2026 if this rule creates hardship
- Confirm your billing team has reviewed the FY 2027 consolidated billing code list
- Track the advance care planning RFI for future QRP inclusion
- Plan for all-payer MDS expansion ahead of FY 2031 SNF QRP
- Set up real-time views for MDS completion, QRP status, and VBP scores
- Note snapshot dates for DC Function and Major Injury (Long-Stay) measures
Frequently Asked Questions
What is the FY 2027 SNF Proposed Rule?
It is CMS’s annual update to Medicare payment policies for skilled nursing facilities. It covers SNF PPS payment rate changes, wage index updates, SNF QRP and SNF VBP program changes, consolidated billing updates, and requests for input on PDPM and advance care planning. CMS released it on April 2, 2026. The official CMS fact sheet (CMS-1843-P) lays out every provision. It was entered into the Federal Register on April 7, 2026.
When will the FY 2027 SNF rule become final?
CMS typically releases the final SNF rule in late July or early August. The FY 2027 final rule is expected by August 2026 and takes effect October 1, 2026. The public comment period closes June 1, 2026.
How will the proposed rule affect SNF reimbursement?
CMS proposes a 2.4% increase to SNF PPS rates, adding an estimated $888 million across all SNFs for FY 2027. The CMS SNF PPS — the prospective payment system — is the federal model that sets Medicare’s daily rate for skilled nursing care. Your net payment will depend on your SNF VBP scores, your local wage index, and whether you meet all SNF QRP rules. Missing QRP rules triggers a two-percentage-point cut to your Annual Payment Update.
What is case-mix creep under PDPM?
Case-mix creep is when patient coding shifts toward higher-paying groups over time — without a matching rise in care needs. It can happen by accident or on purpose. CMS has tracked this pattern since the Patient-Driven Payment Model launched in 2019. The RFI signals that future PDPM changes may fix it. Audit your coding now.
What is the public comment deadline, and how do I submit?
The deadline is June 1, 2026. Go to regulations.gov and search for Docket ID CMS-1843-P. You can also submit through your state or national group like AHCA/NCAL. Be specific: name the provision, explain the impact on your facility, and propose an alternative if you have one.
What should skilled nursing facilities do now?
Start with a payment model: rate update + VBP score + wage index. Then audit your MDS workflows and PDPM coding for case-mix creep. Strengthen your patient intake and care coordination steps. Review the FY 2027 consolidated billing code list. And file public comments before June 1, 2026 if this rule creates real hardship.




















