
Table of Contents
Key Takeaways
- Interoperability isn’t just IT, its revenue strategy.
When data doesn’t flow, you get denials, duplicate tests, prior auth delays, and silent revenue leakage. Fix the flow, and financial performance improves. - Standards help, but architecture wins.
HL7 and FHIR are table stakes. What really matters is a modern integration layer, strong governance, and clean patient identity management. - Modern integration is a competitive edge.
Connected systems mean smoother care, cleaner claims, stronger patient trust, better security, and real readiness for value-based care.
Introduction: The Interoperability Gap in Modern Healthcare
Healthcare interoperability is the ability of different healthcare systems, applications, and devices to exchange, interpret, and use data in a coordinated way that supports patient care, operations, and reporting. Healthcare interoperability is not just about moving data; it is about making that data understandable and actionable wherever a patient shows up.
However, persistent healthcare interoperability challenges continue to prevent systems from sharing data reliably across EHRs, labs, billing platforms, and patient engagement tools.
Interoperability sits at the center of patient safety, clinician experience, revenue cycle performance, and healthcare cost containment strategies. When health records, insurance data, imaging, labs, and digital health tools cannot talk to each other, the result is delayed decisions, duplicate testing, revenue leakage, and frustrated patients who lose trust in their providers.
Despite billions invested in EHRs and health information exchange programs, interoperability remains one of healthcare’s biggest operational bottlenecks.
Studies show that poor electronic health record (EHR) interoperability drives duplicate testing, denials, and administrative waste across U.S. hospitals and physician practices.
This guide explains:
- What healthcare interoperability really means
- Why interoperability is so hard to achieve
- How it affects both clinical outcomes and financial performance
- A practical roadmap for solving interoperability challenges using modern healthcare integration software.
What Is Healthcare Interoperability?
As already discussed, healthcare interoperability means that health information can move securely and accurately between different systems so clinicians, payers, and patients all see a consistent, up‑to‑date picture of care. Effective healthcare data interoperability allows EHRs, practice management systems, labs, imaging centers, pharmacies, payers, and digital health applications to work together as if they were one unified system.
Interoperability is not only technical; it is also about process and policy. True healthcare IT interoperability ensures that data flows at the right time, to the right person, in the right format, and under the right privacy and security rules.
Levels of Interoperability in Healthcare
Experts often describe three core levels of interoperability in healthcare:
- Foundational interoperability – The most basic level. Systems can send and receive data but may not interpret it in the same way. For example, a lab system transmits a PDF to an EHR, but the receiving system cannot parse or structure the data.
- Structural interoperability – Data is exchanged in a structured, standardized format (for example, HL7 messages or FHIR resources), so receiving systems can parse specific fields like medications, allergies, or lab values.
- Semantic interoperability – The highest level. Systems not only exchange structured data but also share the same meaning (for example, using standard vocabularies such as SNOMED CT, LOINC, or RxNorm), enabling clinical decision support and analytics across settings.
Most organizations have achieved some degree of foundational and structural healthcare data interoperability but still struggle with semantic alignment and consistent clinical data exchange across vendors and care settings.
The Regulatory Push: ONC Interoperability Rules and The 21st Century Cures Act
In the United States, the Office of the National Coordinator for Health Information Technology (ONC) sets certification standards and ONC interoperability rules to push vendors and providers toward open, connected systems. The 21st Century Cures Act’s interoperability and information blocking provisions require certified health IT developers, health information exchanges, and providers to avoid practices that unreasonably restrict access, exchange, or use of electronic health information.
Key Themes In The Cures Act and ONC’s Cures Act Final Rule Include:
- Expanding patient access to electronic health information (EHI) via standardized APIs.
- Reducing information blocking by EHR vendors and health information exchange networks.
- Promoting adoption of modern API standards, such as FHIR, to support digital health interoperability and patient-facing apps.
Regulation has accelerated progress, but it has not fully solved the many real‑world EHR interoperability challenges that healthcare leaders face day to day.
Why Interoperability Remains a Challenge
TL; DR:
Top Healthcare Interoperability Challenges:
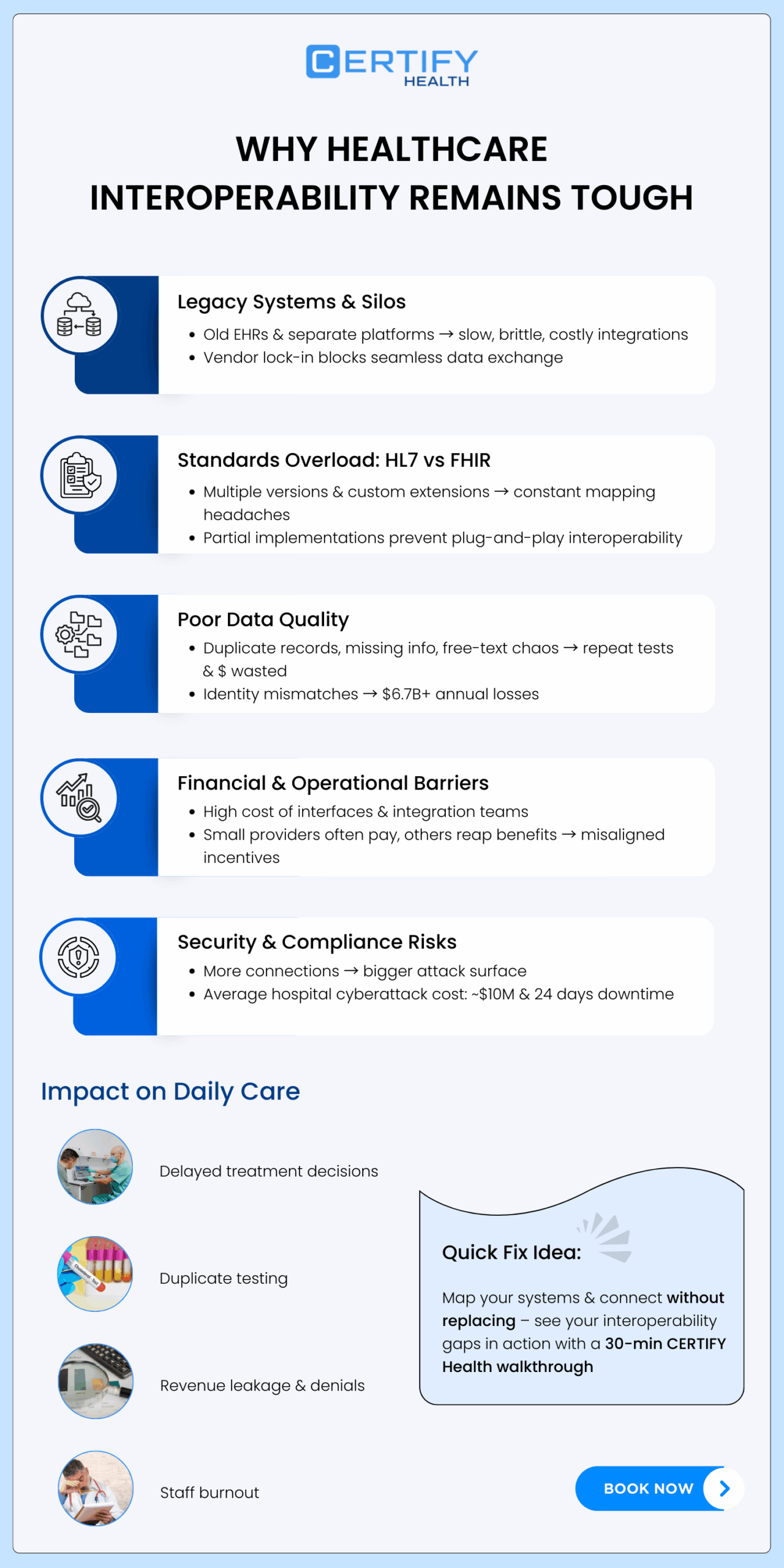
- Legacy systems and EHR silos make integration slow, fragile, and expensive.
- HL7 vs FHIR complexity means most organizations must juggle multiple standards and versions at once.
- Poor data quality and identity mismatches drive duplicate testing, denials, and millions in avoidable costs.
- Financial misalignment makes interoperability hard to justify, even when the long-term ROI is clear.
- Cybersecurity risks increase with every new connection, raising concerns about downtime and breach exposure.
Even with clear definitions, technical standards, and regulatory pressure, healthcare interoperability remains stubbornly difficult. Healthcare data integration is constrained by aging infrastructure, inconsistent standards, uneven data quality, misaligned incentives, and healthcare cybersecurity risks that grow with every new connection.
The following subsections break down the major healthcare IT interoperability barriers and how they show up in daily operations.
1. Legacy Infrastructure and EHR Silos
Many hospitals and health systems still run a patchwork of legacy systems, multiple EHRs across service lines, separate billing platforms, niche specialty applications, and home‑grown tools that were never designed for modern healthcare system integration. These older systems often lack mature APIs or use proprietary interfaces that make healthcare data integration slow, brittle, and expensive.
Vendor lock‑in compounds the problem. When critical workflows depend on a single EHR’s proprietary tools, organizations fear that pushing too hard on open healthcare interoperability will disrupt clinical operations or trigger costly upgrades. In practice, this leads to “good enough” point‑to‑point interfaces that handle a subset of messages but do not deliver true end‑to‑end clinical data exchange.
For multi‑hospital systems or large physician groups that have grown through mergers, EHR interoperability challenges can be even worse. Different sites may use different EHRs or versions, and without a cohesive healthcare integration software strategy, each new connection becomes another custom project.
2. Inconsistent data standards: HL7 vs FHIR and beyond
Standardization is supposed to make healthcare data interoperability easier, but the real‑world picture is more complicated. HL7 Version 2 has been used for decades to transmit lab results, ADT messages, and orders, but local customizations and optional fields mean that one organization’s HL7 feed can look very different from another’s.
FHIR (Fast Healthcare Interoperability Resources) is the newer standard designed for modern APIs and mobile apps, and many refer to the current landscape as HL7 vs FHIR when comparing integration strategies. In reality, most organizations must support both HL7 and FHIR, plus older formats such as CDA documents, as they modernize step by step.
Common issues include:
- Multiple versions of FHIR in use (DSTU2, STU3, R4, R5) across vendors.
- Custom extensions that hinder plug‑and‑play digital health interoperability.
- Partial or non‑standard implementations that require heavy mapping to support health information exchange.
Without a deliberate standardization strategy, healthcare IT interoperability efforts become a constant battle against mismatched schemas and idiosyncratic interfaces.
3. Data quality and semantic gaps
Even when technical connections exist, poor data quality and semantic inconsistencies undermine interoperability. Common healthcare data quality issues include duplicate patient records, missing allergies, outdated problem lists, inconsistent use of diagnosis codes, and free‑text documentation that cannot be easily searched or analyzed.
A study found that 32 percent of transferred patients experienced duplicate testing within 12 hours due to lack of EHR interoperability, and 20 percent of those duplicate tests were not clinically indicated. These findings highlight how incomplete or inaccessible data drives unnecessary utilization and costs.
Identity matching is another major challenge. The Journal of AHIMA found that mismatched patient identities can lead to duplicated tests and procedures, increasing costs by nearly $2,000 per hospital stay and $1,700 per emergency visit, with over one-third of denied insurance claims linked to these errors, amounting to more than $6.7 billion in annual losses across the U.S. healthcare system.
Without strong healthcare data governance, a robust master patient index, and clear healthcare data stewardship practices, even the best technical connections will not deliver reliable, longitudinal records for clinical decision‑making.
Many organizations now implement a formal data governance framework healthcare leaders can use to standardize definitions, enforce data quality rules, and establish consistent data stewardship best practices across clinical, operational, and financial systems.
4. Financial and operational barriers
Building and maintaining interfaces, mapping data, and managing upgrades require significant investment in integration teams and healthcare integration software. Many smaller providers, behavioral health practices, and rural hospitals struggle to fund robust healthcare system integration, even though they bear the same expectations for interoperability as large academic centers.
At the same time, existing payment models do not always reward data sharing. Providers often shoulder the costs of building interfaces, while payers, technology vendors, and downstream partners reap many of the financial benefits. This misalignment makes it hard to justify capital requests for healthcare data interoperability projects unless leaders can connect them directly to revenue protection, healthcare cost containment strategies, or strategic growth.
5. Security and compliance risks
Every new connection, EHR interfaces, FHIR APIs, health information exchange participation, or third‑party app integration, expands the organization’s attack surface. Interoperable EHRs rely on internet‑connected platforms that are inherently vulnerable to cyberattacks if not properly secured.
An analysis of cyberattacks on interoperable electronic health records reported that the average hospital downtime after an attack was 24 days, with an average cost of about 10 million dollars per incident. Another review of healthcare cybersecurity challenges noted that while the 21st Century Cures Act promotes interoperability and patient access, more work is needed on cybersecurity policies to match the growing risk of large‑scale data breaches.
This reality makes some organizations hesitant to expand digital health interoperability, even though secure integration is often safer than ad‑hoc workarounds like emailing spreadsheets or faxing sensitive information.
See how your systems really connect
Book a 30‑minute walkthrough with CERTIFY Health to map your interoperability gaps, and see what “connected without replacing” could look like for your EHR stack.
Impact Summary: Clinical And Financial Consequences
When healthcare interoperability falls short, the impact is felt on both the clinical and financial fronts:
- Delayed care: Clinicians wait for external records, or repeat patient histories manually, delaying diagnosis and treatment decisions.
- Duplicate testing: Lack of health information exchange and poor healthcare data integration lead to repeat labs and imaging; American studies link incomplete record transfer and non‑interoperable systems to high rates of unnecessary duplicate tests.
- Revenue leakage healthcare: Identity mismatches, missing eligibility data, and inconsistent documentation drive denials and underpayments, costing billions annually.
- Burnout and administrative burden: Staff spend hours chasing data across portals and faxes instead of relying on unified healthcare interoperability.
Operational Impact of Healthcare Interoperability Challenges
While interoperability is often discussed as a technical issue, the real consequences appear in daily healthcare workflows. When systems cannot exchange patient data seamlessly, operational friction spreads across nearly every step of the care journey.
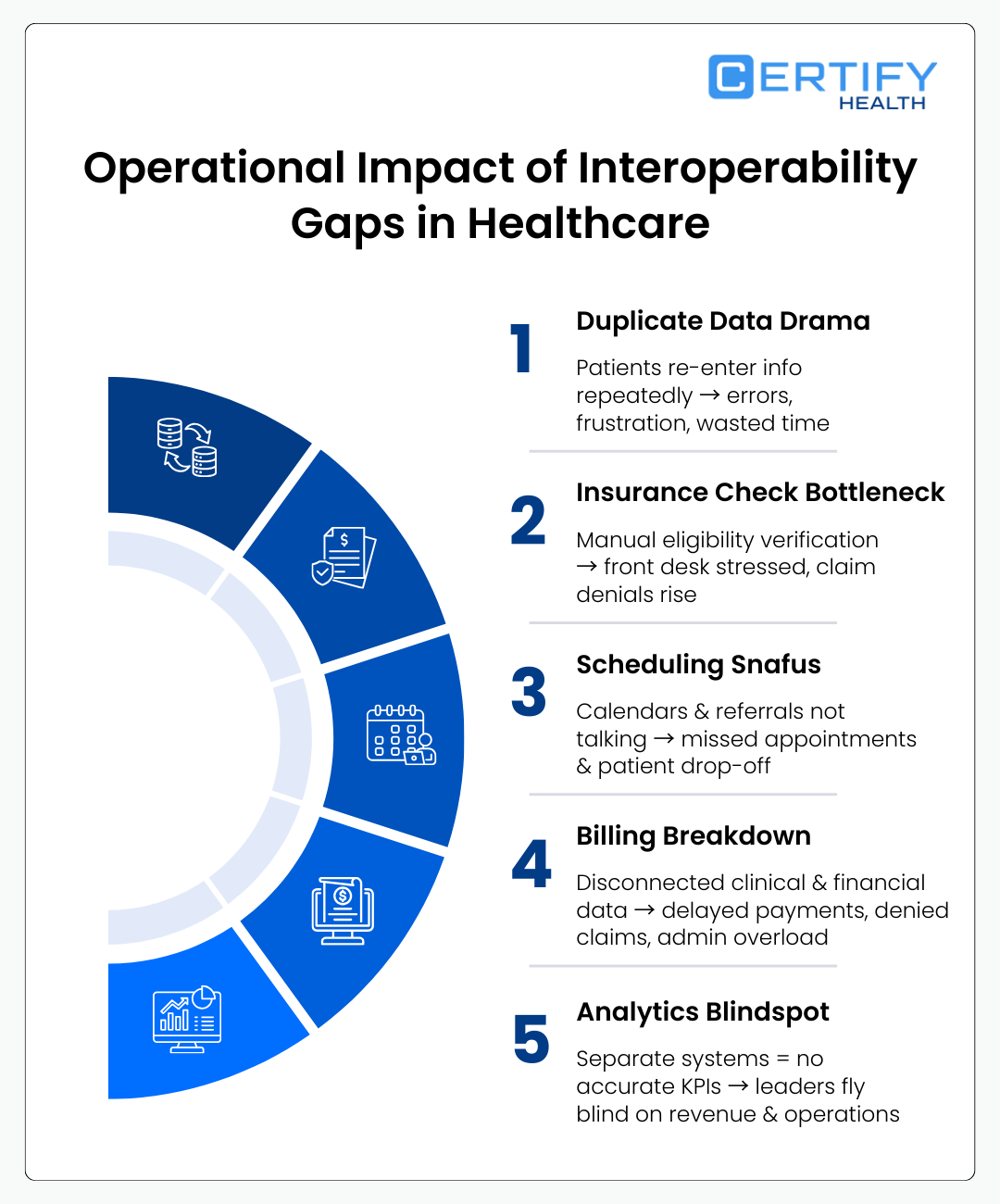
Patient Intake Duplication
Without connected systems, patients repeatedly enter the same demographic and medical history information across portals, forms, and check-in kiosks. This duplication increases registration errors and undermines patient experience.
Delay in Eligibility Verification
Disconnected payer interfaces prevent real-time eligibility verification automation. Staff must manually check insurance portals, increase front-desk workload and raising the risk of coverage errors that later become claims denials and rework.
Disconnected Scheduling Systems
When scheduling systems are not integrated with referral networks or EHR calendars, appointment coordination becomes manual. This leads to referral leakage, long scheduling cycles, and patient drop-off before care begins.
Fragmented Billing and Payment
Fragmented billing systems create gaps between clinical documentation, coding, and payment capture. Missing or inconsistent data often surfaces later as claim denials, delayed reimbursements, or additional administrative rework.
Reporting and Analytics Gaps
Operational leaders struggle to build reliable performance dashboards when clinical, financial, and engagement systems store data separately. Without unified data pipelines, healthcare organizations lack accurate reporting on KPIs such as denial rates, patient throughput, or revenue leakage healthcare metrics.
Why Traditional Integrations and Healthcare Integration Engines Fall Short
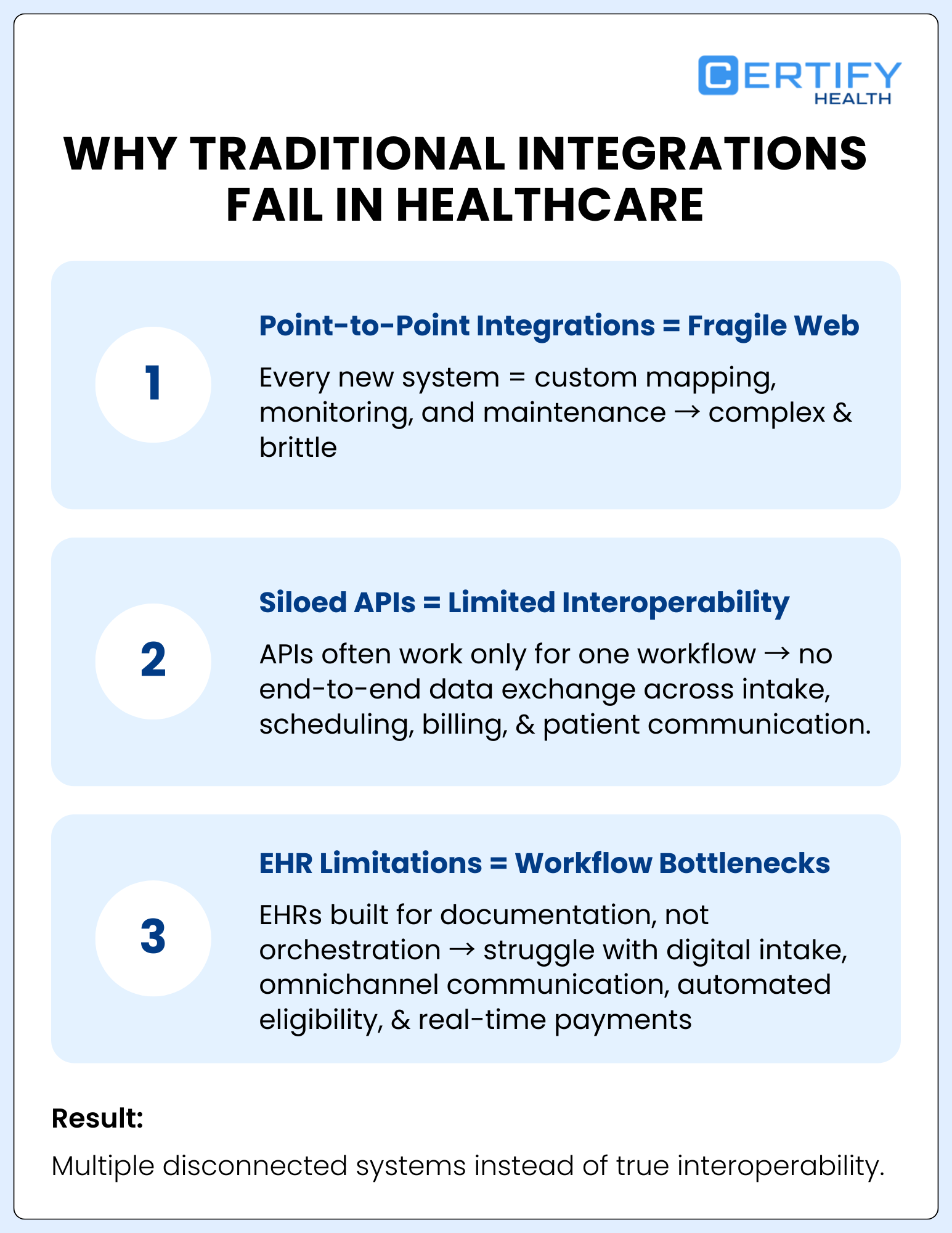
Many organizations attempt to solve healthcare interoperability challenges by deploying traditional integrations or healthcare integration engines. While these tools can connect systems technically, they often fail to solve workflow fragmentation.
Point-to-Point Integrations Create Fragile Ecosystems
Traditional interface engines rely heavily on point-to-point integrations between systems. Every new application requires custom mapping, monitoring, and maintenance, creating an increasingly complex web of dependencies.
Siloed APIs Limit Real Interoperability
Even when vendors expose APIs, they frequently operate as isolated endpoints tied to specific workflows. These siloed APIs rarely support full lifecycle data exchange across intake, scheduling, eligibility, billing, and patient communication workflows.
EHR Platform Limitations
Many EHR platforms were originally designed as documentation systems, not workflow orchestration platforms. As a result, they struggle to manage modern interoperability needs such as digital intake, omnichannel communication, automated eligibility checks, and real-time payment workflows.
Without broader vendor and platform alignment for FHIR adoption, organizations often end up managing multiple disconnected integrations rather than achieving true healthcare data interoperability.
How Interoperability Impacts Financial Performance
TL; DR:
The Financial Impact of Poor Interoperability
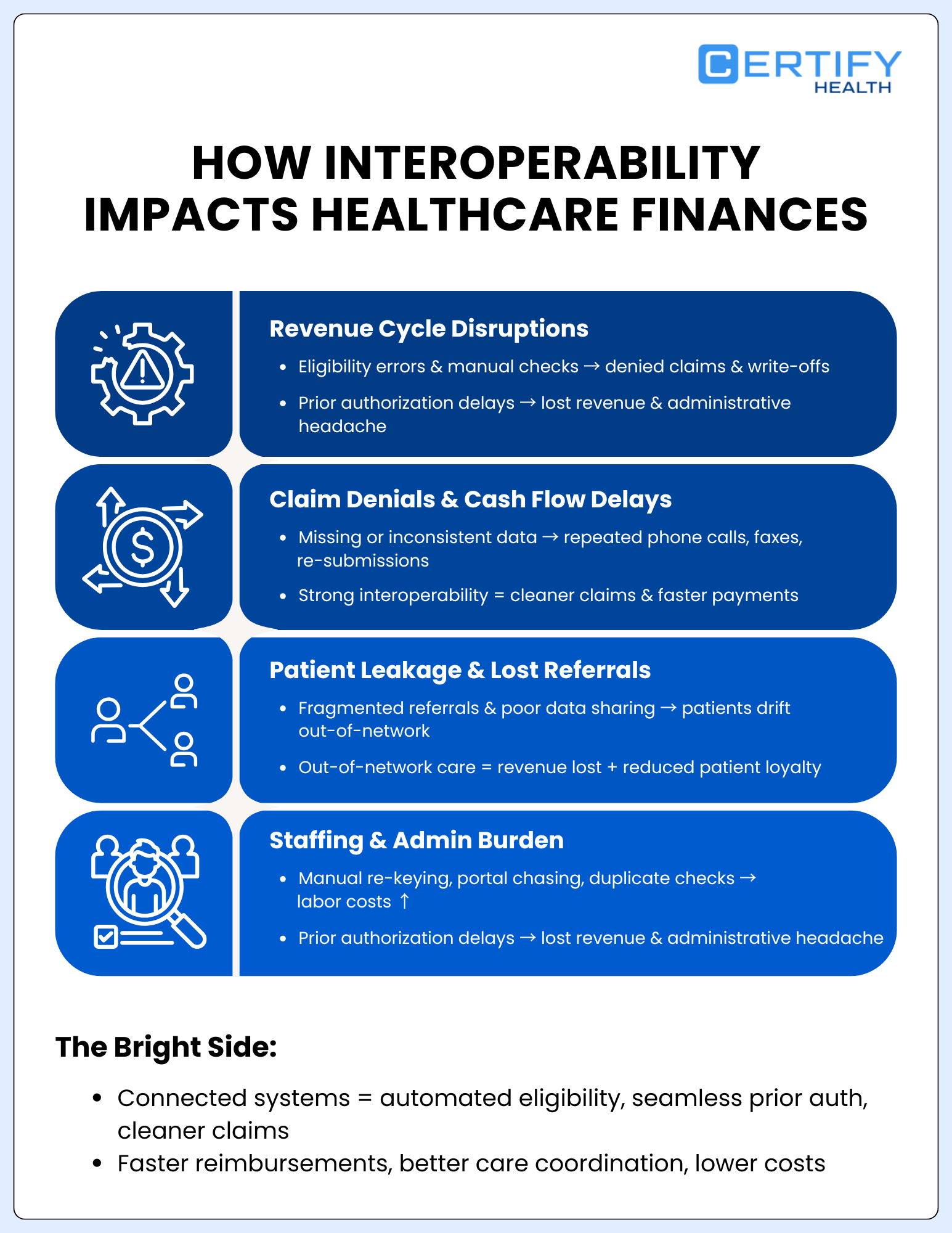
- Interoperability gaps directly hurt revenue cycle performance. Eligibility errors, missing data, and manual workflows lead to denials, write-offs, and delayed cash flow.
- Prior authorizations break down without clean data exchange. When clinical documentation and status updates don’t flow electronically, delays and avoidable denials increase.
- Poor connectivity drives patient leakage. Fragmented referrals and weak data sharing push patients out of network — and revenue goes with them.
- Manual work inflates staffing costs. Re-keying data, chasing records, and managing portals consume valuable time and labor.
- Strong interoperability protects margins. Clean data flow supports cleaner claims, faster payments, better care coordination, and sustainable cost containment.
Interoperability is often framed as a clinical or IT problem, but its financial footprint is just as large. Poor healthcare interoperability and fragmented healthcare data integration directly affect revenue cycle performance, cash flow, and cost structures across provider organizations.
A. Revenue Cycle Disruptions
Healthcare revenue cycle workflows, eligibility checks, pre‑authorization, coding, billing, and payment posting, depend on timely, accurate data flowing between EHRs, practice management systems, clearinghouses, and payer portals. When healthcare interoperability is weak, gaps appear at every step.
Eligibility verification gaps and automation opportunities
If demographic or coverage data cannot flow reliably between registration systems, payers, and EHRs, front‑desk staff often rely on manual eligibility checks or outdated insurance information. These breakdowns in eligibility verification automation lead to coverage errors, write‑offs, and denied claims.
Interoperable eligibility feeds and payer APIs can automate much of this work, but only if healthcare system integration is designed to capture and reconcile payer responses back into the EHR and billing system.
Claim denials and prior authorization delays
Prior authorization and medical necessity reviews are particularly sensitive to interoperability failures. A JAMA Health Forum analysis estimated that the annual cost of prior authorization requirements to U.S. physicians ranges from 1.3 billion to 26.7 billion dollars, driven by administrative time and workflow disruption. When clinical data, documentation, and authorization status cannot be exchanged electronically, staff resort to phone calls, faxed forms, and manual uploads into payer portals.
These barriers create a vicious cycle of delayed decisions, care deferrals, and denied claims. Denial management is expensive, and industry surveys show that a large share of initial denials is eventually overturned on appeal, meaning the root problem is often missing or inaccessible data rather than true ineligibility.
By contrast, strong healthcare IT interoperability and payer integration support automated prior authorization status checks, structured documentation sharing, and cleaner claim submission.
B. Care coordination and patient leakage
Fragmented healthcare interoperability makes it harder to coordinate referrals, follow‑up, and chronic disease management across networks. When specialists, primary care providers, labs, and imaging centers cannot easily share data, patients may drift to out‑of‑network providers who offer more seamless digital experiences.
Lost referrals and out‑of‑network utilization contribute to revenue leakage healthcare organizations can ill afford. Identity errors and incomplete clinical data also lead to missed opportunities for follow‑up visits, preventative screenings, and care gap closures that drive value‑based incentives and patient loyalty in healthcare.
C. Administrative burden and staffing costs
Poor interoperability multiplies manual tasks: downloading records from external portals, re‑keying lab results, reconciling duplicate patients, and tracking prior authorizations by spreadsheet. Qualitative research on interoperability challenges has shown that hospitals and health information exchanges see substantial staff time consumed by managing interfaces, reconciling data, and working around information blocking or incomplete feeds.
As labor costs rise and clinical staff shortages grow, these inefficiencies are untenable. Investing in high‑quality healthcare interoperability becomes a core part of healthcare cost containment strategies, not just an IT upgrade.
The Cost of Poor Interoperability
The costs of weak healthcare interoperability show up in three main categories: direct IT costs, indirect operational and clinical costs, and strategic costs that affect long‑term competitiveness.
Direct IT and integration costs
Direct costs include:
- Custom interface development and maintenance across dozens of systems.
- Ongoing upgrades, testing, and vendor coordination for each new integration.
- Licensing and infrastructure for legacy integration engines that were not designed for modern digital health interoperability.
Organizations that rely on bespoke point‑to‑point connections often spend disproportionate IT budgets just keeping the lights on, leaving little room for innovation.
Indirect operational and clinical costs
Indirect costs are often larger and more hidden (as already mentioned earlier):
- Duplicate testing and procedures: Research shows that incomplete EHR interoperability leads to high rates of duplicate tests; one study found that 32 percent of transferred patients had repeat tests within 12 hours, with 20 percent not clinically indicated.
- Identity and documentation errors: AHIMA’s analysis documented that mismatched patient identities add nearly 2,000 dollars to every hospital stay and 1,700 dollars per emergency visit on average, with more than 6.7 billion dollars in annual costs tied to denied claims from these errors.
- Cybersecurity incidents: Cyberattack analyses report average hospital downtime of 24 days and an average cost of about 10 million dollars per incident when interoperable EHRs are compromised.
From a cost‑containment perspective, improving healthcare data interoperability and addressing healthcare cybersecurity risks can pay for themselves by reducing avoidable waste and risk.
Strategic and competitive costs
Strategic costs are often overlooked but substantial:
- Lost competitive positioning: Health systems that lag on digital health interoperability struggle to support digital front doors, remote monitoring, and data‑driven population health initiatives.
- Reduced patient loyalty healthcare: Patients expect their records to follow them. When they repeatedly fill out the same forms or experience visible data gaps, trust erodes and they may seek more digitally mature competitors.
- Inflexibility for value‑based care: Advanced value‑based arrangements require reliable, timely data flows across providers and payers; weak interoperability makes it hard to manage risk and demonstrate outcomes.
Even a simple, conservative cost model, adding up a fraction of duplicate testing, denials attributable to documentation gaps, and the expected cost of a cybersecurity incident, shows that poor healthcare interoperability can quietly drain millions each year from a mid‑size organization.
Also, Read: Why Healthcare Interoperability Matters and How to Build It
How to Overcome Interoperability Challenges: A Solution Framework
TL; DR:
A Practical Framework to Fix Healthcare Interoperability
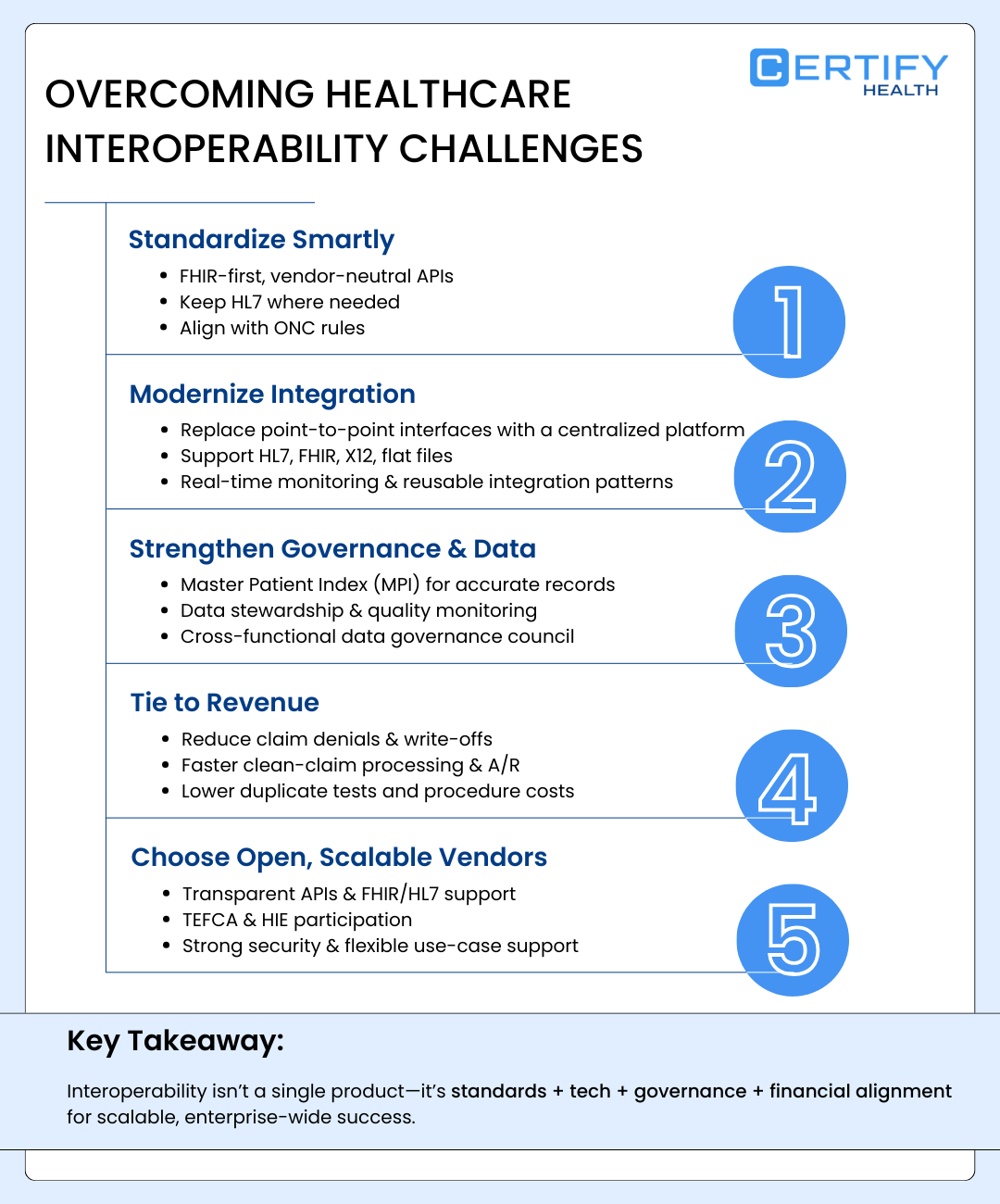
- Standardize smartly: Use FHIR-first, vendor-neutral architecture while supporting HL7 where needed.
- Modernize integration: Replace point-to-point interfaces with a centralized integration platform.
- Strengthen governance: Implement an MPI, data stewardship, and quality monitoring.
- Tie to revenue: Connect interoperability to denials, clean claims, A/R, and cost reduction KPIs.
- Choose open partners: Prioritize secure, standards-based vendors aligned with long-term scalability.
Solving healthcare interoperability is not about buying a single product. It is about combining standards, technology, governance, and financial alignment into a coherent healthcare data integration strategy.
The following solution framework can help leaders move from scattered pilot projects to a scalable, enterprise‑wide approach.
1. Standardization Strategy: Move Toward FHIR‑first, Vendor‑neutral Design
A clear standardization strategy is the foundation for sustainable healthcare interoperability.
Key actions include:
- Adopt FHIR‑based APIs where possible: Prioritize interfaces that expose normalized FHIR resources for core domains (patients, encounters, observations, medications, coverage) while maintaining HL7 feeds where needed. This avoids a false choice of HL7 vs FHIR and instead uses each where it fits best.
- Design vendor‑neutral architecture: Avoid hard‑coding workflows to any single vendor’s proprietary interface. Instead, use an abstraction layer that can map data across systems and vendors.
- Align with ONC interoperability rules: Ensure certified health IT and partner platforms support standardized API access and avoid information blocking behaviors.
This standardization strategy closes the gap between regulatory intent and real‑world healthcare IT interoperability.
2. Integration Layer Modernization: From Point‑to‑point To Platform
Rather than building one‑off interfaces between every pair of systems, leading organizations invest in a modern integration layer, middleware or healthcare integration software that centralizes mappings, monitoring, and error handling.
A robust integration platform should:
- Support HL7, FHIR, X12, flat files, and other formats used in clinical data exchange and financial transactions.
- Provide real‑time monitoring, alerting, and replay for failed messages.
- Offer reusable integration patterns for common use cases like lab orders/results, eligibility verification automation, prior authorization, and health information exchange.
This approach reduces the long‑term cost and complexity of healthcare system integration and makes it easier to onboard new partners or applications.
3. Governance, Data Strategy, And Stewardship
Technology alone cannot fix interoperability if underlying data is unreliable. Strong governance and healthcare data stewardship are essential.
Key components include:
- Healthcare data governance council: A cross‑functional group (IT, clinical, compliance, revenue cycle) that sets standards, approves data definitions, and prioritizes interoperability initiatives.
- Master patient index (MPI): A robust MPI uses probabilistic matching and standardized identifiers to reduce duplicate records and mismatches that drive costs and safety risks.
- Data quality management: Ongoing monitoring of key indicators such as duplicate rates, missing fields, and coding consistency helps address healthcare data quality issues before they impact clinical or financial outcomes.
With this foundation, semantic interoperability and reliable analytics become achievable goals rather than aspirational buzzwords.
4. Revenue Alignment: Tie Interoperability To RCM KPIs
To sustain investment, healthcare interoperability projects must be tied to clear financial outcomes. Leaders should explicitly link initiatives to revenue and cost metrics such as:
- Reduction in claim denial rates tied to missing or inconsistent data.
- Improved clean‑claim rates and faster days in A/R.
- Lower write‑offs from coverage errors through better eligibility verification automation.
- Reduced duplicate testing and procedure costs.
Framing interoperability as a lever for healthcare cost containment strategies and revenue protection helps secure executive sponsorship and prioritization.
5. Vendor evaluation criteria and ecosystem design
Finally, organizations must choose partners and platforms that share their vision for open, secure healthcare interoperability.
Vendor criteria should include:
- Transparent, well‑documented APIs and support for FHIR and HL7.
- Demonstrated participation in national health information exchange networks and TEFCA alignment where applicable.
- Strong security posture, including robust controls to mitigate healthcare cybersecurity risks.
- Flexibility to support diverse clinical and financial use cases without forcing a rip‑and‑replace of existing core systems.
Read: Before You Implement Healthcare Interoperability Solutions, Read These 10 Critical Factors
Connect your ecosystem without touching your core EHR
Request a Tailored Demo to see how quickly your team could move from point‑to‑point interfaces to a unified integration fabric.
CERTIFY Health: A Unified Platform for Interoperable Healthcare Workflows
Addressing healthcare interoperability challenges requires more than technical integrations. It requires a unified operational platform that connects fragmented workflows across the patient journey.
CERTIFY Health’s healthcare interoperability software is designed to help organizations “connect without replacing,” acting as an operations and engagement layer that wraps around existing EHRs and practice management systems.
Instead of simply connecting systems, CERTIFY Health unifies critical operational workflows including:
- Digital patient intake and insurance capture
- Appointment scheduling and referral coordination
- Automated eligibility verification
- Patient interaction and experience management
- Healthcare billing and payment administration systems
By connecting these workflows, CERTIFY Health helps eliminate the operational fragmentation that often sits behind healthcare interoperability challenges.
Through standards-based integration using HL7 and FHIR APIs, the platform synchronizes these workflows with existing EHR systems while preserving the clinical record as the system of record.
This unified workflow architecture helps:
- Eliminate intake duplication
- Streamline eligibility verification automation
- Reduce claims denials and rework
- Provide operational visibility across the entire patient journey
Instead of forcing organizations to pick sides in the HL7 vs FHIR debate, CERTIFY Health acts as a healthcare data integration and orchestration layer that normalizes data across formats and systems.
See how CERTIFY Health connects 234+ EHRs without disruption.
Interoperability Implementation Roadmap
TL; DR:
How to Roll Out Interoperability Without Disrupting Operations
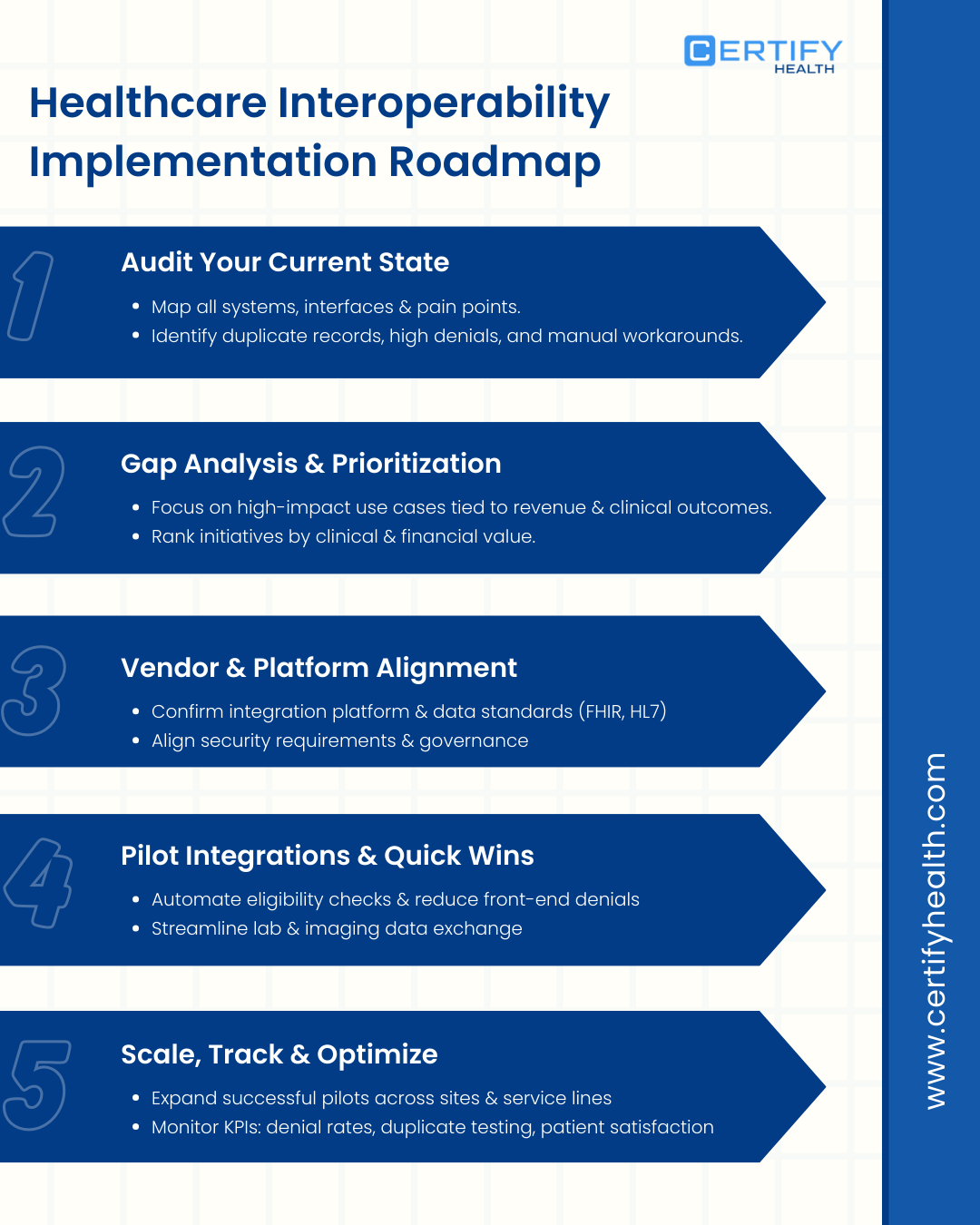
- Audit your current state: Map every system, interface, and pain point.
- Prioritize what matters: Focus on high-impact use cases tied to revenue and clinical outcomes.
- Align vendors and standards: Confirm integration platform, data standards, and security expectations.
- Start with quick wins: Pilot targeted integrations with measurable KPIs.
- Scale and optimize: Expand successful use cases and continuously track performance improvements.
Once a strategy is defined and a capable interoperability partner is in place, organizations need a realistic implementation roadmap. The following five‑phase approach provides a high‑level structure that can be adapted to different sizes and settings.
Phase 1: Current state audit
In this phase, leaders take inventory of:
- All clinical, financial, and ancillary systems that participate in healthcare data interoperability.
- Existing interfaces, including HL7 feeds, FHIR APIs, batch file exchanges, and manual workarounds (such as portals and faxes).
- Known EHR interoperability challenges, such as duplicate patient records, high denial rates tied to data gaps, or recurring failures in clinical data exchange.
The goal is to build a single view of the current integration landscape, including technical diagrams and process maps.
Phase 2: Gap analysis and prioritization
Next, the team compares the current state to desired future capabilities for healthcare interoperability.
Key questions include:
- Where are the most critical pain points? (For example, referral leakage, prior auth delays, revenue leakage healthcare, or cybersecurity exposure.)
- Which use cases deliver the highest combined clinical and financial value if improved?
- How do current systems support or hinder digital health interoperability goals, such as patient apps or remote monitoring?
This phase results in a prioritized roadmap of interoperability use cases, each linked to clear outcomes and KPIs.
Phase 3: Vendor and platform alignment
With priorities established, organizations work to align vendors and internal teams around a coherent healthcare system integration approach.
Activities include:
- Selecting or confirming an enterprise integration platform or healthcare integration software.
- Defining data standards and governance expectations with vendors (for example, FHIR resources supported, HL7 implementation guides followed).
- Aligning security requirements to minimize healthcare cybersecurity risks while enabling necessary data flows.
For many providers, this is where a partner like CERTIFY Health can accelerate progress by bringing pre‑built connectors and proven integration patterns to bear.
Phase 4: Pilot integrations and quick wins
Organizations should begin with a focused set of pilots that address visible pain points and prove the value of healthcare interoperability.
Examples include:
- Automating eligibility verification automation and coverage checks to reduce front‑end denials.
- Streamlining lab and imaging clinical data exchange between the EHR and external partners.
- Integrating digital intake or patient engagement tools so data flows directly into the EHR without re‑keying.
Each pilot should have clear metrics, for example, reduction in duplicate tests, improvement in clean‑claim rate, or decreased time to schedule a follow‑up visit.
Phase 5: Scale, KPI tracking, and optimization
After successful pilots, the focus shifts to scaling integrations across more sites, service lines, and partners.
Key activities include:
- Expanding interoperability use cases based on the roadmap.
- Monitoring KPIs such as denial rates, duplicate testing rates, and patient satisfaction to quantify the impact of improved healthcare interoperability.
- Continuously refining data quality processes, healthcare data stewardship roles, and governance to sustain gains.
The Future of Interoperability in Healthcare
Looking ahead, healthcare interoperability will not be a one‑time project but an ongoing capability that underpins digital transformation.
Real‑time data exchange and event‑driven care
Interoperability is also moving from batch exchanges to real‑time, event‑driven architectures. Instead of nightly file transfers, modern healthcare IT interoperability uses FHIR subscriptions, event hubs, and streaming platforms to support immediate updates to care teams, payers, and patients.
This real‑time clinical data exchange will support:
- Proactive outreach when results indicate urgent follow‑up is needed.
- Event‑driven care coordination, such as automatic alerts to primary care when a patient is discharged from the ED.
- Faster financial events, like instant eligibility verification and point‑of‑service estimates.
Value‑based care, consumer expectations, and regulation
Value‑based payment models, consumer‑grade digital expectations, and evolving ONC interoperability rules all point in the same direction: more transparent, secure, and fluid health information exchange.
Organizations that invest in robust healthcare interoperability now will be better positioned to:
- Compete on patient experience and patient loyalty in healthcare.
- Thrive in value‑based contracts that demand cross‑organizational data sharing.
- Adapt quickly as new digital health interoperability mandates and technologies emerge.
Bottomline
Healthcare interoperability challenges are not just technical problems. They create real operational and financial friction across healthcare organizations.
When systems cannot exchange patient data effectively, the impact appears immediately in daily workflows: duplicate patient intake, eligibility verification delays, disconnected scheduling, fragmented billing, and reporting gaps. These inefficiencies drive claims denials and rework, higher administrative costs, and poor patient experiences.
Solving these issues requires more than traditional integrations or interface engines. Healthcare organizations need unified workflow platforms that connect intake, scheduling, eligibility, communication, and payments while integrating with EHRs through HL7 and FHIR standards.
Platforms like CERTIFY Health help transform interoperability from a technical integration problem into a connected operational architecture that improves both patient experience and financial performance.
Explore how CERTIFY Health’s interoperability platform connects your EHR, RCM, and patient experience tools, or Book a 30‑minute Demo.
Frequently Asked Questions (FAQs)
Define What is interoperability in healthcare?
Healthcare interoperability is the ability of different healthcare systems, such as EHRs, labs, and billing platforms, to exchange, interpret, and use patient data securely across organizations.
It ensures clinicians, payers, and care teams can access accurate patient information at the right time, supporting coordinated care and operational efficiency.
Why are healthcare interoperability challenges so common?
Healthcare interoperability challenges occur because many organizations rely on legacy EHR systems, inconsistent data standards, and fragmented integrations.
Poor healthcare data governance, identity mismatches, and siloed workflows across labs, payers, and scheduling systems also make reliable clinical data exchange difficult.
How do healthcare systems exchange patient data?
Healthcare systems exchange patient data using interoperability standards and integration technologies.
Common methods include HL7 messages, FHIR APIs, Clinical Document Architecture (CDA), health information exchanges (HIEs), and secure data integration platforms that synchronize records across providers and payers.
What role do healthcare integration engines play?
Healthcare integration engines connect healthcare systems by routing, transforming, and translating data between applications.
They help move information across platforms like EHRs, labs, and billing systems, but many rely on point-to-point integrations, which can still leave operational workflows fragmented.
How does interoperability impact revenue cycle performance?
Poor interoperability disrupts revenue cycle workflows by creating eligibility verification errors, missing documentation, and delayed prior authorizations.
These gaps often lead to claims denials and rework, slower reimbursements, and higher administrative costs for healthcare organizations.




















